 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 65, No. 3, May-June, 2003, pp. 282-284 Papillary carcinoma arising in a thyroglossal duct remnant Kamal Kant, Girish Rajpal Department of Surgery, Dr. S. N. Medical College, Jodhpur, Rajasthan, India.
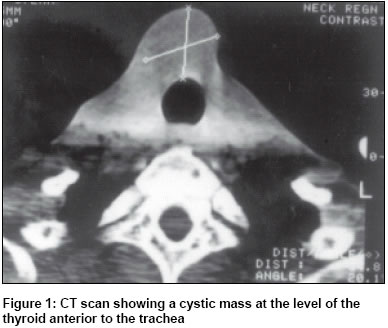
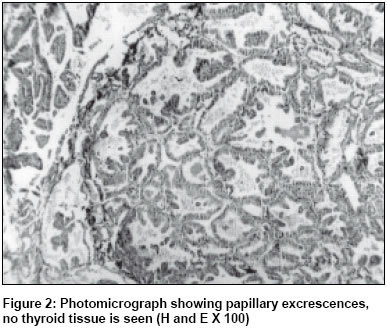
Paper Received: April 2002. Paper Accepted: June 2002. Source of Support: Nil Code Number: is03058 ABSTRACT Carcinoma arising in the congenital thyroglossal duct remnant is a rare occurrence. Less than 150 cases are reported in the literature, most being papillary carcinoma. We report a papillary carcinoma arising in a thyroglossal duct remnant in a 50-year-old man. Management of this condition remains controversial. Most of these tumours arise from the ectopic thyroid tissue within the cyst. Prognosis is good as long as there is no metastasis. Sistrunk procedure is adequate if histology does not reveal extracystic extension. KEY WORDS: Papillary carcinoma, Thyroglossal duct remnant. How to cite this article: Kant K, Rajpal G. Papillary carcinoma of thyroglossal duct remnant. Indian J Surg 2003;65:282-4. INTRODUCTION Thyroglossal duct cyst is the most common congenital anomaly that arises from the remnants of the thyroglossal duct. The thyroglossal duct descends from the base of the tongue into the neck by the seventh week of the intrauterine life. Less than 150 cases of carcinoma occurring in the thyroglossal duct remnant have been reported worldwide.1 The thyroid gland in all these cases remained normal except in 4 cases in which there was postoperative diagnosis of carcinoma of the thyroid after thyroidectomy.1 As such, experience in dealing with this condition is limited and management remains controversial. We report a 50-year-old man with papillary carcinoma arising in a thyroglossal duct remnant and review the literature. CASE REPORT A 50-year-old man was admitted with complaints of a painless spherical swelling in the region of the hyoid bone that was noticed 2 years ago. The swelling moved with swallowing and upon protrusion of the tongue. The swelling had remained static in size for a long time. There was no associated cervical lymphadenopathy. A computerized tomogram showed a cystic mass (Figure 1) separate from the thyroid gland. At surgery, a solid mass was found attached partially to the cricoid cartilage and separate from the isthmus of the thyroid. Both lobes of the thyroid were normal. The tumour was excised in-toto leaving behind an intact thyroid gland. The patient made an uneventful recovery. Histopathology revealed it to be papillary carcinoma but no thyroid follicles were seen (Figure 2). DISCUSSION Thyroglossal duct cysts are the most common non-odontogenic cysts in the neck, estimated to occur in 7% of the adult population.2 They are usually located in the midline or less frequently in the lateral anterior region of the neck. The incidence of papillary carcinoma arising in the thyroglossal duct cyst is < 1%. The diagnosis is often made postoperatively on histological examination of the resected specimen. The age of presentation ranges from 6 to 81 years with an average age of 39 years. Clinical presentation is similar to that of benign cysts. Women are affected more commonly than men. Primary carcinoma arising from the epithelium lining the cyst has been described in a few cases.3 Metastases were mentioned in only 7.7% of cases. Possible sites for these metastases are ovary, breast, gastrointestinal tract and thyroid. There are two schools of thought about the origin of these tumours which forms the basis of therapy. The first school of thought considers these tumours to be metastases from occult thyroid carcinoma that may have undergone cystic degeneration.4 These authors advocate subtotal or total thyroidectomy with neck dissection. The current concept in the literature is against such radical surgery unless there is associated abnormality in the thyroid gland or cervical lymph node metastases are present. Most authors consider a Sistrunk's operation to be adequate as the majority of these tumours appear to have their origin in the ectopic thyroid tissue present within the thyroglossal cyst.1 Careful histological examination is important to differentiate between these tumours and metastases that have undergone a cystic degeneration. The major criteria include high cellularity, the presence of papillary formations, and cells with enlarged nuclei with anisonucleosis and powdery chromatin with definite nucleoli. Intranuclear pseudoinclusions and grooves are the significant diagnostic criteria. Psammoma bodies, multinucleated giant cells, and ropy colloid are variably present.5 If the tumour has not extended beyond the cyst wall, histologically normal ectopic thyroid tissue is seen, the thyroid gland is normal and if the cervical lymph nodes are not present local excision is adequate. If the carcinoma is shown to extend beyond the capsule a wider excision is necessary. All patients, whether they undergo thyroidectomy or not, should receive sufficient doses of T4 to suppress the secretion of TSH as the differentiated tumours are stimulated by TSH. The prognosis of papillary carcinoma is good whether it occurs in the thyroglossal duct cyst or in the thyroid gland proper. REFERENCES
Copyright 2003 - Indian Journal of Surgery. Also available online at http://www.indianjsurg.com The following images related to this document are available:Photo images[is03058f2.jpg] [is03058f1.jpg] |
| |||||||||

{kind=link}
{kind=link}