 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
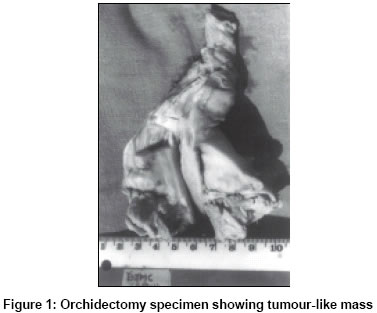
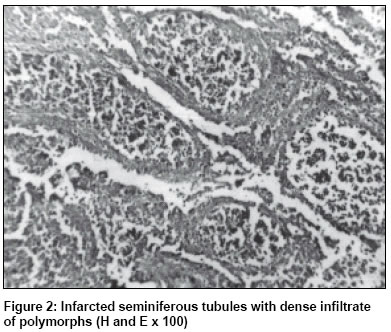
Indian Journal of Surgery, Vol. 65, No. 3, May-June, 2003, pp. 284-285 Case Report Testicular infarction clinically mimicking a neoplasm Sujata Nayak, Shaila. C. Puranik, Vasudev V. Holla Department of Pathology, B. J. Medical College and Sassoon General Hospital, Pune 411001, India.
Paper Received: Februray 2002 Paper Accepted: Septemebr 2002 Source of Support: Nil Code Number: is03059 ABSTRACT Testicular infarction presenting as a tumour-like mass is rare. A case of orchidectomy performed in a young male with this entity is described. KEY WORDS: Testes, Infarct. How to cite this article: Nayak S, Puranik SC, Holla VV. Testicular infarction clinically mimicking a neoplasm. Indian J Surg 2003;65:284-5. CASE REPORT An 18-year-old male presented with a grayish white firm mass in the left testis of size 4x3x3 cm which was present since 6 weeks. The mass was protruding beyond the tunica vaginalis (Figure 1). A vague history of trauma was given by the patient. Preoperative laboratory investigations were within normal limits. An orchidectomy was performed with the clinical impression of testicular tumour. Multiple histological sections were studied which revealed necrosed seminiferous tubules heavily infiltrated by polymorphs and a few eosinophils (Figure 2). No normal testicular tissue was seen. Epididymis also showed a similar inflammatory infiltrate. A histological diagnosis of testicular infarct was given. DISCUSSION Testicular infarction clinically simulating a neoplasm is a rare entity. To the best of our knowledge there are less than 20 reported cases.1-4 Due to the rarity of this entity it was usually not considered in the differential diagnosis preoperatively. Use of scrotal ultrasonography also did not help distinguish cases of infarct from a tumour.3-5 A more recent publication however, mentions the use of high-frequency colour Doppler ultrasound as a reliable method of diagnosing testicular infarction.6 Testicular infarction may be segmental or global. Most reported cases are segmental.1-3,5 Global infarction, as has occurred in the present case, is usually secondary to torsion of the testis around the spermatic cord. Other causes include haematological disorders like leukaemia, sickle-cell anaemia, compression of blood vessels by hernia or tumour, thromboembolism and vasculitis. An irreversibly damaged testis is best resected. An early orchidectomy prevents adverse effects on spermatogenesis in the contralateral testis and also helps exclude malignancy by histological confirmation. However, in cases of segmental infarction preoperative diagnosis can allow testis-sparing surgery.4-6 REFERENCES
Copyright 2003 - Indian Journal of Surgery. Also available online at http://www.indianjsurg.com The following images related to this document are available:Photo images[is03059f2.jpg] [is03059f1.jpg] |
| |||||||||

{kind=link}
{kind=link}