 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
| ||
|
Indian Journal of Surgery, Vol. 65, No. 4, July-Aug, 2003, pp. 325-336 Review Article Conservative surgery in breast cancer Indraneel Mittra, R. A. Badwe, K. Dinshaw,1 R. Sarin,1 R. C. Chinoy,2 R. Nair,3 M. Thakur,4 V. Parmar, R. Hawaldar5 Departments of Surgical Oncology, 1Radiation Oncology,
2Surgical Pathology, 3Medical Oncology,
4Radio-diagnosis and 5Clinical
Research Secretariat, Tata Memorial Hospital, Ernest Borges Road, Parel, Mumbai 400012.
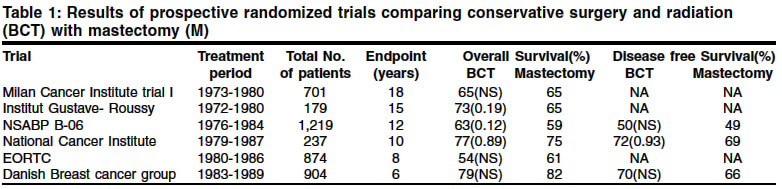
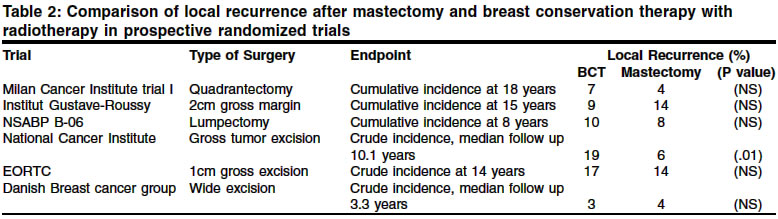
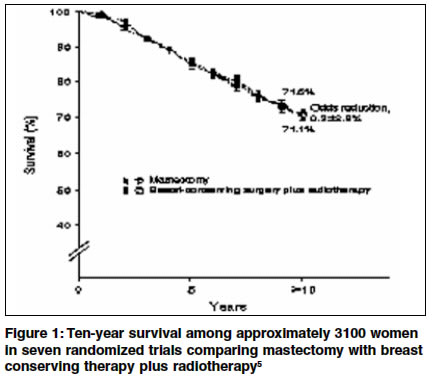
Paper Received: June 2002. Paper Accepted: November 2002. Source of Support: Nil How to cite this article: Mittra I, Badwe RA, Dinshaw K, Sarin R, Chinoy RC, Nair R, et al. Conservative surgery in breast cancer. Indian J Surg 2003;65:325-35. Code Number: is03066 Abstract Breast conservation surgery (BCS) has become a standard treatment for early breast cancers with results equivalent to modified radical mastectomy (MRM) as evident from various randomized trials. Based on available evidence, the Breast Unit at Tata Memorial Hospital (TMH) has also evolved a standard protocol for the management of breast cancer. The proportion of cases undergoing BCS in operable breast cancer has shown a significant upward trend from 12.6 % in the year 1997 to 59.3% in the year 2001. In operable breast cancer, the overall incidence of gross positive cut margin has been 4 % after BCS. With encouraging results in early breast cancer, BCS is also being offered to women with larger, locally advanced breast cancer (LABC) after downsizing with neo-adjuvant chemotherapy. In 1997, 0.4% of LABC had breast conservation as compared to 34% in the year 2001. The gross positive margin rate in LABC after BCS was 2.4% in our patients (p=0.43). The local recurrence rate after BCS in our patients was 2% in both operable breast cancer (15 out of 726 women) and locally advanced cancers (2 out of 101 women). Even as conservative surgical treatment in early breast cancer is fast becoming the gold standard, conservative radiotherapy to tumour bed alone is also under study. Presently, radical radiotherapy to whole breast plus tumour bed boost is the standard protocol for all women after BCS. A feasibility study of conservative radiotherapy with a high dose brachytherapy for tumour bed alone in early breast cancer is presently on at TMH with a close collaboration between the departments of Breast Services Surgical Oncology and Radiation Oncology with early morbidity as the end-point. Key Words Breast conservation surgery, Operable breast cancer, Locally advanced breast cancer. Introduction Evidences from the past: Randomized clinical trials Breast conservation surgery is fast becoming the gold standard for early breast cancer although mastectomy still remains appropriate for some patients. With the maturing of results from various randomized trials of more extensive surgery versus less extensive surgery, conservative surgery has gained popularity all over the world. The initial results of the NSABP trial of radical mastectomy vs. mastectomy with or without radiation published in 1985,1 showed no significant survival difference between the axilla treated and untreated groups indicating that the extent of local treatment alone did not influence the outcome. No systemic chemotherapy was used in this trial. Six prospective randomized trials were carried out comparing mastectomy with conservative surgery and radiation between the 1970s and 1980s2 for stage I and stage II breast cancer. The Milan Cancer Institute, Institut Gustave-Roussy, NSABP-B06, National Cancer Institute, EORTC 10801 and the Danish Breast Cancer Group carried out these trials. In all these trials, adjuvant systemic chemotherapy was used in node positive patients. Whole breast irradiation was administered with a boost to the primary tumour site in all except the NSABP B-06 trial.3 The results of these trials showed that radical mastectomy and breast conservation surgery have equivalent therapeutic benefits in terms of overall survival (Table 1). The incidence of ipsilateral breast tumour recurrence (IBTR) after conservation and irradiation was 3-19%, as compared to 4-14% incidence of chest wall recurrence after mastectomy. All the trials had a prerequisite of clear resection margins excepting the National Cancer Institute trial4 in which only a tumorectomy was practised and which reported the highest local recurrence rate of 19% in the conservation group (Table 2). A recent meta-analysis of nine prospective randomized trials5 comparing mastectomy with conservative surgery and radiation published in 1995, again showed no difference in overall survival at 10 years in seven of these trials (Figure 1). There was a 6.2% local recurrence rate in mastectomy patients and 5.9% in breast conservation. In the node positive women, wherein more than 50% receive postoperative radiotherapy (RT) after mastectomy, there was no difference in survival. However, within the node negative cancers, where fewer than 50% receive RT after mastectomy, breast conservation treatment (BCT) had a significantly better survival with routine RT being administered to all patients (odds ratio 0.69, p=0.003).
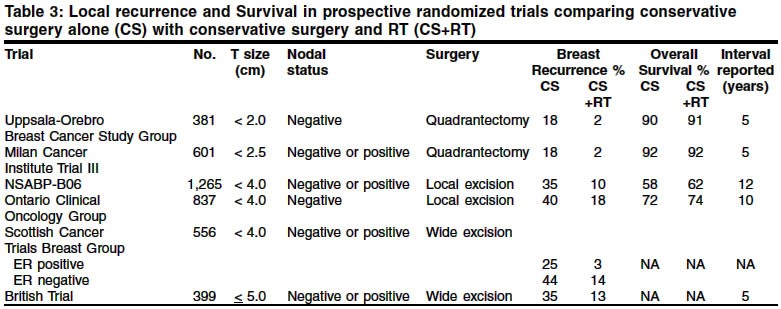
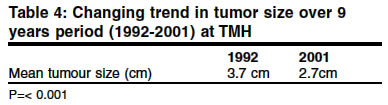
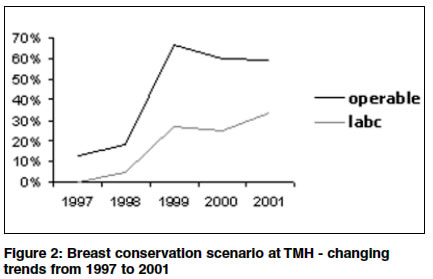
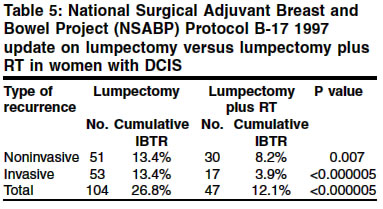
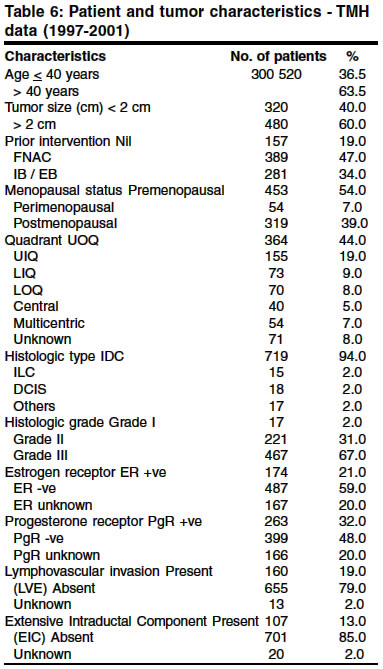
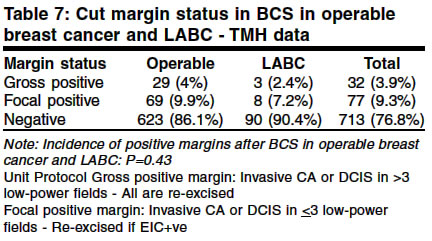
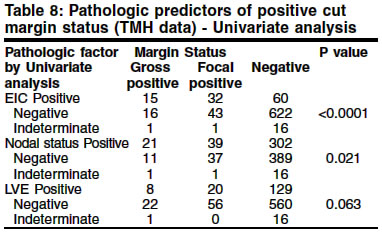
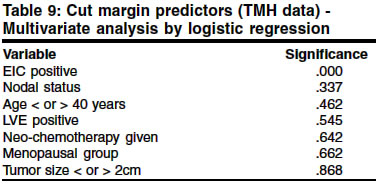
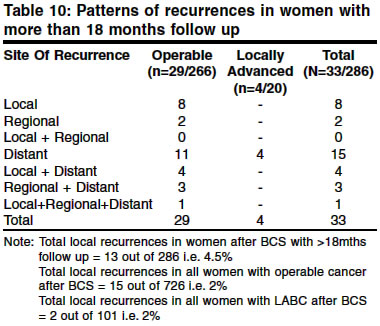
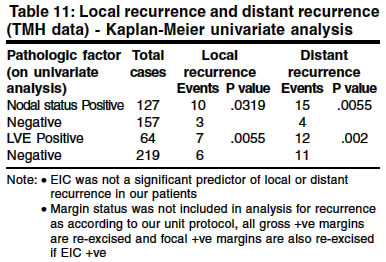
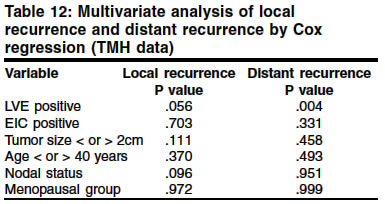
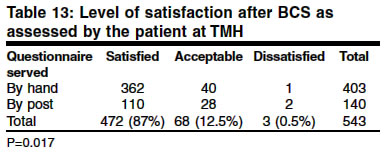
The Institut Gustave-Roussy trial6 found that most recurrences appeared during the first 10 years. Overall survival, distant metastasis, contralateral breast cancer, new primary malignancies, and loco-regional recurrence rates were similar in both mastectomy and breast conservation. Role of radiotherapy in breast conservation There have been six randomized trials in the past comparing radiation vs. no radiation in breast conservation.2 A clear benefit from radiation therapy was noted with an average reduction in the rate of local recurrence by 84% (range 73-97%). The NSABP B-06 trial (total mastectomy vs. lumpectomy vs. lumpectomy with radiation) showed that the cumulative incidence of recurrence of tumour in the ipsilateral breast was 35% in the group treated with lumpectomy alone as compared to 10% in the group treated with lumpectomy and breast irradiation (p<0.001) at 12 years follow-up.7 There was no difference in the overall survival and distant disease-free survival rates in the three groups (Table 3). Ipsilateral breast tumour recurrence (IBTR) following BCT Even as breast conservation surgery gained popularity, the problem of local recurrence after conservation became a prime issue as it indicated a failure of procedure. The possible predictive and prognostic factors for local recurrence after BCT were extensively studied to reduce the incidence of IBTR. Various retrospective studies have analyzed the possible high risk factors for increased incidence of local and distant recurrences after conservation surgery and radiation. These included young age, premenopausal status, adequacy of excision and margin status, multifocal or multicentric disease, lymphovascular emboli, tumour size, lymph node status, negative estrogen receptors, and other histological features like high-grade tumour necrosis, infiltrating lobular histology, and mononuclear cell reaction. Younger age has been variously implicated in higher local failures after breast conservation8-10 while other series have found age not to be predictive of local or regional relapses.11 In univariate analysis, premenopausal status was associated with higher local relapses but the significance was lost in multivariate analysis.10 Similarly, negative estrogen receptor status,12,13 large tumour size,13 high-grade tumours,11,14 intralymphatic tumour extension10,15 and infiltrating lobular histology14 have also been shown to be independent predictors of loco-regional relapses. The term extensive intraductal component (EIC) was coined by Schnitt et al16 for moderate or marked intraductal cancer in the primary tumour and intraductal cancer involving grossly normal surrounding breast tissue. They found a higher relapse of 52% in EIC positive tumours with 6000cGy of tumour bed irradiation compared to 16% recurrence when the tumour bed dose was > 6000cGy. Other investigators have also reported a higher risk of local recurrence after conservation in the presence of EIC within the primary tumour,8,17 while a few have reported no such correlation with EIC.11,15 The lack of consistency regarding the significance of EIC could be explained by differences in treatment policies among various institutions, association with other unfavourable histological factors and variability in defining EIC. Lindley et al17 studied histological features in loco-regional relapses in 293 patients with BCT and reported that when intraductal carcinoma comprised 25% or more of the tumour, there was an increased risk of locoregional failure (p = 0.003). Holland et al18 concluded that higher rates of recurrences occurred in patients with breast conservation with EIC positive tumours due to a larger subclinical tumour burden in the remainder of the breast as compared to tumours that do not contain EIC. The residual tumour was predominantly ductal carcinoma in situ (DCIS). Obtaining an adequate surgical excision and obtaining clear margins prior to radiotherapy in conservative surgery has been shown to reduce local recurrence rates. After a randomized study of quadrantectomy vs. lumpectomy in small size breast cancers, Veronesi et al19 observed a local recurrence rate of 2.2% and 7% respectively. Ghossein et al20 also compared the extent of excision (tumorectomy vs. wide excision vs. quadrantectomy) prior to radiotherapy in 503 patients and observed the local recurrences rates. Involved margins were 41% in tumorectomy, 14% in wide excision and 7% in quadrantectomy, with a corresponding rate of local failures of 15%, 7% and 5% respectively (P <0.03). Surgical margin status after lumpectomy has also been shown to be a predictor of long-term local recurrence in other studies.22 However, the largest trial, the NSABP experience, had clearly shown that the extent of excision does not affect disease-free survival and overall survival. The relationship between the microscopic margins of resection, EIC and ipsilateral breast recurrence after breast conservation surgery was subsequently studied21 and presented at the annual meeting of the American Society for Therapeutic Radiology and Oncology at Florida in October 1995. A consensus was arrived at defining a `positive margin'. Any amount of tumour at the margins in a low-power field was considered positive. Positive margins were further classified as focally positive (if invasive or in-situ ductal carcinoma was present at the margins in <3 low-power fields) or more than focally positive (if invasive or in-situ ductal carcinoma was present at the margins in >3 low-power fields). The 5-year IBTR rate for patients with focally positive margins was 9% (9% for EIC-negative and 7% for EIC-positive patients) and for patients with greater than focally positive margins was 28% (19% for EIC-negative and 42% for EIC-positive patients). A re-excision of close, indeterminate, or positive margins with final attainment of negative margins resulted in a significant improvement in local control.21,22 By univariate and multivariate analysis, margin status was a significant predictor (P=0.009) for local recurrence while EIC was not significant (P=0.20) in the presence of clear surgical margins. Significance of local recurrence after breast conservation After a local relapse in conservative management, Cowen et al23 reported a shorter median time to distant metastases with a hazard ratio of 4.4 times, but an early timing of local recurrence did not indicate a higher risk for distant metastases. Local recurrence was merely a marker for propensity for distant metastasis. Factors associated with higher local relapses were histological multifocality, lymphovascular emboli and young age in that order, while distant relapses were associated with tumour size, young age and histological multifocality. Clarke et al11 observed that breast relapses following radiotherapy become clinically apparent more slowly than chest wall failures after mastectomy and if detected early, these patients may be successfully treated. Breast conservation in large tumours The earlier trials of breast conservation in Europe had included only tumours of 2.5 cm or less. The NSABP trial later had included tumours up to 4 cm in size. Presently, if the relative size of the tumour to breast volume is adequate, even larger tumours can be considered for BCS. Preoperative chemotherapy in large operable breast cancers and even in locally advanced tumours can effect a significant decrease in tumour size to allow breast conservation with clear margins. Reducing the size of the primary tumour by chemotherapy before surgery has so far not shown any significant improvement in survival.24 Tumours close to the nipple-areola complex are also no longer an absolute indication for mastectomy and BCS may be performed with a central quadrantectomy. The preserved part of the breast has quite a normal contour and sensation as compared to a reconstructed breast. Contraindications to BCS Pregnancy (first and second trimester), multicentric tumours, and presence of extensive microcalcification on mammogram (indicating presence of DCIS) are absolute contraindications for BCS. Conservation can be offered in small tumours in the third trimester of pregnancy with radiation therapy starting after the delivery. Multifocal tumours may be treated conservatively if limited to a single quadrant. Collagen vascular disorders, ataxia telangiectasia, post-burn scarring and previously irradiated skin tolerate radiation poorly and are relative contraindications for radiation treatment and are patients with any of these conditions are not suitable for BCT. The present scenario: breast conservation treatment at TMH In the west, organized screening programmes for breast cancer have resulted in a significant reduction in the tumour size in women diagnosed with breast cancer. Our own results at TMH also show a reducing trend in the mean tumour size over the past decade (Table 4) from 3.7 cm in 1992 to 2.7 cm in the year 2000 (p<0.001), attributable not to any population-based screening programmes but to an increased awareness of breast cancer. Breast conservation, when not contraindicated, is presently being offered to all eligible women presenting to the Breast Unit at TMH with early operable breast cancer and in large operable and locally advanced breast cancers after downsizing with neo-adjuvant chemotherapy. In the year 1997, the total conservative surgeries numbered 67 out of 515 breast surgeries performed for breast cancer i.e.12.4%. The numbers have steadily increased over the years as shown in Figure 2, with the rate of conservation surgery being 53.2% in June 2001. Treatment is offered based on well-defined evidence-based protocols. From January 1997 up to June 2001 (42 months), 906 breast conservation surgeries have been performed. Fourteen of these women were primarily reconstructed using latissimus dorsi flap. The percentage of primary breast reconstructions has been less due to a more frequent use of neo-adjuvant chemotherapy for downsizing of larger tumours. In women with large operable breast cancer and locally advanced breast cancer (LABC), trials of neo-adjuvant chemotherapy have shown no significant improvement in overall survival.36 Nevertheless, this has resulted in an improvement in the rate of conservation surgery. The TMH figures for BCT in LABC have also increased from 0.4% in 1997 to 34% in 2001 (Figure 2). The overall breast conservation rate in LABC at TMH between the years 1998 to 2001 has been 21%. Technical aspects in BCS The goal of conservative surgical treatment in breast cancer is complete removal of all suspicious or known malignant tissue with a gross clear margin by excising a 1.0-1.5 cm rim of grossly normal breast tissue with a minimal resultant cosmetic deformity. The placement of incision should be directly over the palpable lump with no raising of flaps or tunnelling. In the upper half of the breast, incisions are placed circumferentially while lower half incisions give cosmetically better results if placed radially, especially so if they also require excision of skin. Breast tissue is not re-approximated after the excision. Meticulous haemostasis is a must and no drains are kept at the lumpectomy site. The lumpectomy specimen should always be oriented with sutures (the standard labelling technique being short superior suture, long lateral suture and black silk for anterior surface) to enable pathologists to clearly indicate the status of margin. Routine frozen section reporting is not advised for assessment of margin. Where a previously biopsied site with unknown margin status is re-excised, a 1.0-1.5 cm rim of breast tissue is removed around the previous biopsy site incorporating the previous biopsy scar. The axillary clearance is performed through a separate transverse incision at the lower axillary hairline in a lazy-S fashion starting from the lateral pectoral fold to the fold raised by the lateral border of the latissimus dorsi muscle. Axilla is completely cleared with removal of level III nodes with the laying bare of the axillary vein (but not stripping the whole vein to minimize postoperative arm oedema). The thoracodorsal and long thoracic nerves should be preserved. The medial pectoral nerve should also be preserved and, if feasible, the intercostobrachial nerve may also be preserved. A closed suction drainage of the axilla is always recommended. The cavity of the axillary dissection is isolated from that of the primary tumour cavity if the latter is in the upper outer quadrant for a subsequent better cosmesis. Early postoperative mobilization should be encouraged to minimize a frozen shoulder. Histopathological evaluation The lumpectomy specimen is inked on the outer surface before processing. Gross examination should document size of specimen, size of tumour in three dimensions, and distance of all margins from the tumour. Microscopic evaluation should report the histological type and grade of tumour, presence and extent of DCIS and EIC, the microscopic presence or absence of tumour at the margins, presence or absence of lymphovascular invasion, perineural and perinodal invasion, and lymph node status (total dissected and positive nodes). Immunohistochemistry with reporting of estrogen receptor and progesterone receptor status is also necessary to decide adjuvant systemic therapy. Adjuvant loco-regional and systemic therapy All patients of breast conservation receive radiation therapy to the breast with a boost to the primary tumour bed if the pathological margin status is negative. Positive cut margins are initially classified as gross positive or focal positive. All gross positive cut margins are re-excised. The presence or absence of EIC decides the management of focal positive margins. EIC-negative focal positive cut margins are treated by additional radiation boost to the tumour bed. EIC-positive focal positive cut margins are all re-excised with a few exceptions. Positive anterior margin, posterior margin and peripherally situated tumours with corresponding positive margin are not re-excised due to absent or inadequate residual breast tissue at the site. Re-excision may be in the form of a wider re-excision or a mastectomy depending on the residual breast size and cosmetic acceptability. Patient preference is also considered when deciding about re-excision. Further systemic adjuvant therapy is decided based on the menopausal status, tumour size, nodal status, and presence or absence of hormone receptors as per standard treatment protocols. Diagnosis and management of DCIS Before the widespread use of mammography, DCIS was an infrequently encountered entity that was routinely managed by mastectomy. DCIS is detected mammographically due to the presence of microcalcification though 10% of DCIS may not be associated with calcification. The significance of such localized screen-detected in-situ carcinoma is a matter of debate. DCIS treated by mastectomy alone carries a small risk (0-2%) of relapse. With its evident success in invasive breast carcinoma, BCS is also being considered for the management of localized in-situ carcinoma of breast. Palpable DCIS is managed on the lines of invasive carcinoma. Impalpable DCIS presenting only as microcalcification on mammogram has to be localized by image-directed biopsy and confirmed pathologically to rule out the presence of invasive cancer. Pre-surgical mammography in cranio-caudal and mediolateral views should be performed with localization of the suspicious lesion or microcalcification using a hook wire. The patient is shifted to the operation theatre with the wire in place. The exact location of the lesion should be assessed by triangulation based on the position, angle of wire and the depth of penetration of the wire as estimated by the labelled mammography films. The incision for biopsy of the lesion is placed closest to the tip of the wire avoiding any tunnelling or undermining of skin. The specimen should be labelled as for invasive cancers. The entire specimen should also be radiographed to confirm complete removal of the suspicious lesion. Frozen section reporting of the needle-localized calcification is not advisable as it is difficult to distinguish between atypical ductal hyperplasia and DCIS on frozen section preparations and areas of microinvasion may be completely missed. Margin assessment of needle-localization specimens is also necessary to ensure complete excision of the lesion. The incidence of axillary node metastases in pure DCIS is 0-1%, but in situation of associated palpable mass with a high suspicion of microscopic invasion level I clearance may be performed. The NSABP protocol B-17 trial25 was a prospective randomized trial evaluating the role of RT after lumpectomy for patients with DCIS and clearly confirmed a reduction in IBTR of both invasive and non-invasive cancer, by RT. The trial showed a 26.8% incidence of recurrence in DCIS treated by excision alone with 50% of these recurrences being of invasive nature (Table 5). With the inclusion of RT after lumpectomy, the non-invasive IBTR reduced from 13.4% to 8.2% (p=0.007) and invasive IBTR reduced from 13.4% to 3.9% (p<0.0001). Other randomized trials have also confirmed the benefit of RT in DCIS treated by conservative surgery.26 The role of tamoxifen in DCIS is still under study. The NSABP B-24, which randomly assigned patients undergoing excision of DCIS and irradiation to either placebo or tamoxifen, has shown that tamoxifen further reduces recurrence of DCIS.27 TMH results of breast conservation surgery Material and methods Between January 1997 and June 2001, 906 women underwent BCS at the Breast Unit at TMH. 827 women who had surgery before 1 March 2001 and had completed their adjuvant therapy were included in the present analysis. Out of 827 patients, 726 women had presented with primary operable breast cancer and 101 were locally advanced at presentation. The pertinent clinical characteristics of the 827 women operated are shown in Table 6. The various patient-related and tumour-related predictors of positive margin status were tested by chi-square test for univariate analysis, and by logistic regression analysis for multivariate analysis. Only those patients who had completed 18 months from the date of surgery were analyzed for local recurrence, distant recurrence, and survival. Univariate and multivariate analysis of potential prognostic factors for local recurrence and distant recurrence were performed using the Kaplan-Meier survival analysis and Cox regression models for the whole group. The margin status was reported as negative in 713 cases (86.2%), gross positive in 32 cases (3.9%) and focal positive in 77 cases (9.3%). In the remaining 5 cases the margin status could not be assessed and was labelled as indeterminate. There was 4.0% gross margin positivity in operable breast cancer and 2.4% women were reported to have gross positive cut margins in locally advanced breast cancer (Table 7). Pathological predictors of positive margin on univariate analysis (Table 8) were the presence of EIC and positive nodal status with a significant value of p<0.0001 and p=0.021 respectively. Presence of lymphovascular emboli (LVE) was not found to be a significant predictor for positive cut margin. On multivariate analysis only EIC remained as a strong predictor of positive cut margin (Table 9). Only those patients who had a minimum of 18 months of follow-up after surgery were included for analysis of local recurrence. 286 women had more than 18 months of follow-up. 34 of these women had developed a recurrence; 13 were local recurrences (4.5%) with 8 being only local failures while 5 were with regional or distant failures (none in locally advanced); 6 recurred regionally and there were 23 distant recurrences (4 in locally advanced cases). In one patient the site of the first recurrence was not known at the time of death. The actual pattern of distribution of metastases is shown in Table 10. The potential prognostic factors for local recurrence and distant recurrence were analyzed both by the Kaplan Meier survival tables in univariate analysis and by the Cox model in multivariate analysis. The following variables were evaluated: age < or > 40 years, menopausal status, tumour size, nodal status, presence of EIC and LVE. Both LVE and a positive nodal status were associated with increased incidence of local recurrence and distant recurrence (Table 11). The multivariate analysis by the Cox regression model did not indicate any significant predictor for local recurrence. However, the presence of LVE had a significant impact on distant metastases with a p value of 0.004 (Table 12). The extent of wide excision in women with LABC at initial presentation who undergo BCT after downsizing with neo-adjuvant chemotherapy is the same as that for operable breast cancer. There was a margin positivity rate of 9.6% in the women with LABC as compared to 13.9% positive margin status in the women with operable breast cancer undergoing BCT (Table 11). The difference observed is statistically insignificant with a p value of 0.43. Patient perception of satisfaction after breast conservation surgery There has been a significant increase in the proportion of breast conservation surgeries being performed in the Breast Unit at TMH over the past 4 years. It is essential to perform an audit at regular intervals to ensure satisfactory results. It is also important to know whether the decision to conserve the breast is equally justified and acceptable to the patient. A Quality of life study at the Breast Unit in 300 consecutive cases of operable breast cancer did show that the body image is better preserved in women undergoing BCS as compared to those who have a mastectomy (p=0.0001). This difference is maintained even after completion of adjuvant therapy i.e. after 6 months, indicating that coping skills in mastectomy patients are inadequate in helping to accept the altered body image and BCT is definitely a better option. At the Breast Unit, a patient satisfaction survey was carried out between January 2001 and July 2001 in 543 women who had undergone BCT since 1997. Questionnaires were handed out to some of the women on routine follow-up at the outpatient department while a few questionnaires were sent by post. Answers were obtained pertaining to the woman's level of satisfaction with the appearance and feel of the affected breast following BCS and RT, by selecting one of the three options given, i.e. satisfied, acceptable or dissatisfied. It was interesting to note that 87% of women were satisfied with the appearance of their breast in spite of a difference in the size and feel of the affected breast as compared to the opposite normal breast (Table 13). There was no difference in the levels of satisfaction between the private and general category of patients (probably suggesting that socio-economic status and education may not have a significant role in the psychological reaction of the patient to the type of surgery). However, there was a significant difference between answers obtained to questionnaires sent by post and those handed out to the women attending the outpatients department on regular follow-up (p=0.017). More women were dissatisfied when the reply was sent through post (21.4%) as compared to the questionnaire answers given by hand (10.2%). A similar observation has been made in other studies of patients' health related quality of life after radical prostatectomy, with a significant difference between the perception as evaluated by the treating urologist and as reported by the patient.35 In all domains urologists underestimated patients symptoms. The extent of the margin of excision was documented in 406 patients. The average maximum margin of excision was 2.8 cm while the average least margin of excision was 1.08 cm. The largest margin of surgical excision was compared with the level of satisfaction with BCS to find out if larger lumpectomy or wider excisions were related to a higher cosmetic dissatisfaction. There was no statistically significant correlation between the maximum excision margin width and level of satisfaction with BCS, further validating our treatment protocols for the extent of excision. High dose radical implant in early operable breast cancer Whole breast irradiation followed by an additional boost dose to the tumour bed has been a standard RT protocol after BCT. The irradiation of the entire breast is based on the presumption that the disease may be multicentric in some patients. Most of the local recurrences after BCT are also in the index quadrant15 hence obviating the need for additional boost to the tumour bed. The usefulness of a boost dose over and above whole breast irradiation will be evident only after the EORTC trial37 results mature and become available. The early results only show a poorer cosmesis with boost. Boost may be delivered by means of an electron beam or by an interstitial or brachytherapy implant. The brachytherapy implant offers an advantage due to lesser dosage exposure to the skin. The breast recurrence rates after conservation surgery and radiotherapy are approximately 10%, and 65-90% of these are in the index quadrant in the immediate vicinity of the tumour bed.15 It thus appears that only 1-3.5% of relapses are in remote areas of the breast, thus questioning the requirement for whole breast irradiation. In a prospective randomized trial at Manchester comparing megavoltage radiation to encompass the whole breast and regional nodes (WF) vs. electron field directed to the tumour bed only (LF)38, there was an increased rate of breast recurrence in the limited field group (25% in LF vs 13% in WF group, p=0.00008) with no difference in the overall survival. Only two factors were found significant when the differences in radiotherapy techniques were allowed for—histological grade and lymphovascular invasion. There was also a very high incidence of invasive lobular cancers in the LF group. Therefore, if the high-risk groups are excluded, there should be no difference in the local recurrence rates as well as the overall survival between the LF and WF groups. Following early encouraging results from some prospective studies39,40 the Radiation Therapy Oncology Group (RTOG) has started a multi-institutional trial, RTOG 95-17 of radical TBRT(tumour bed radiotherapy) with LDR/HDR Ir-192 implant in early breast cancer, the results of which are still awaited. Presently, at TMH, there is a feasibility study being carried out for a high dose brachytherapy in early breast cancer with tumours smaller than 4 cm (excluding the high-risk women with ILC or LVE positive tumours) by placement of catheters in the tumour bed at the time of lumpectomy. High dose radical RT is then administered to the tumour bed for a period of 7-10 days. The results of this pilot study are still awaited. Acknowledgement The authors wish to thank the Department of Clinical Research Secretariat at TMH for their assistance in data recording, monitoring and analysis without which it would not have been possible to publish this paper. They also thank Ms. Sunita S. Konapte, data entry operator in the Breast Unit for her sincere efforts in entering and updating the data of patients included in the analysis. References 1. Fisher B, Redmond C, Fisher ER, Bauer M, Wolmark N, Wickerham DL, et al. Ten-year results of a randomized clinical trial comparing radical mastectomy and total mastectomy with or without radiation. N Eng J Med 1985;312;674-81. 2. Winchester DP, Cox JD. Standards for diagnosis and management of invasive breast carcinoma. CA Cancer J Clin 1998;48:83-107. 3. Fisher B, Redmond C, Poisson R, Margolese R, Wolmark N, Wickerham L, et al. Eight-year results of a randomized clinical trial comparing total mastectomy and lumpectomy with or without irradiation in the treatment of breast cancer. N Eng J Med 1989;320:822-8. 4. Jacobson JA, Danforth DN, Cowan KH, d'Angelo T, Steinberg SM, Pierce L. Ten-year results of a comparison of conservation with mastectomy in the treatment of stage I and stage II breast cancer. N Eng J Med 1995;332:907-11. 5. EBCTCG - Effects of radiotherapy and surgery in early breast cancer: An overview of randomized trials. N Eng J Med 1995;333:1444-55. 6. Arriagada R, Monique G Lê, Rochard F, Contesso G. Conservative treatment versus mastectomy in early breast cancer: Patterns of failure with 15 years of follow-up data. J Clin Oncol 1996;14:1558-64. 7. Fisher B, Anderson S, Redmond CK, Wolmark N, Wickerham DL, Cronin WM. Reanalysis and results after 12 years of follow-up in a randomized clinical trial comparing total mastectomy with lumpectomy with or without irradiation in treatment of breast cancer. N Eng J Med 1995;333:1456-61. 8. Kurtz JM. Factors influencing the risk of local recurrence in the breast. Eur J Cancer 1992;28:660-6. 9. Kim SH, Simkovich-Heerdt A, Tran KN, Maclean B, Borgen PI. Women 35 years of age or younger have higher locoregional relapse rates after undergoing breast conservation therapy. J Am Coll Surg 1998;187:94-5. 10. Fourquet A, Campana F, Zafrani B, Mosseri V, Vielh P, Durand JC, Vilcoq JR. Prognostic factors of breast recurrence in the conservative management of early breast cancer: a 25-year follow-up. Int J Radiat Oncol Biol Phys 1989;17:719-25. 11. Clarke DH, Lê MG, Sarrazin D, Lacombe MJ, Fontaine F, Travagli JP, et al. Analysis of loco-regional relapses in patients with early breast cancers treated by excision and radiotherapy: Experience of the Institut Gustave-Roussy. Int J Radiat Oncol Biol Phys 1985;11:137-15. 12. Yaghan R, Stanton PD, Robertson KW, Going JJ, Murray GD, McArdle CS. Oestrogen receptor status predicts local recurrence following breast conservation surgery for early breast cancer. Eur J Surg Oncol 1998;24:424-6. 13. Stotter AT, Mcneese MD, Ames FC, Oswald MJ, Ellerbroek NA. Predicting the rate and extent of locoregional failure after breast conservation therapy for early breast cancer. Cancer 1989;64:2217-25. 14. Clarke DH, Martinez AA. Identification of patients who are at high risk for loco-regional breast cancer recurrence after conservative surgery and radiotherapy: A review article for surgeons, pathologists, and radiation and medical oncologists. J Clin Oncol 1992;10:474-83. 15. Fisher ER, Sass R, Fisher B, Gregorio R, Brown R, Wickerham L. Pathologic findings from the National Surgical Adjuvant Breast Project (protocol 6) II. Relation of local breast recurrence to multicentricity. Cancer 1986;57:1717-24. 16. Schnitt SJ, Connolly JL, Harris JR, Hellman S, Cohen RB. Pathologic predictors of early local recurrence in stage I and II breast cancer treated by primary radiation therapy. Cancer 1984;53:1049-57. 17. Lindley R, Bulman A, Parsons P, Phillips R, Henry K, Ellis H. Histologic features predictive of an increased risk of early local recurrence after treatment of breast cancer by local tumor excision and radical radiotherapy. Surgery 1989;105:13-20. 18. Holland R, Connolly JL, Gelman R, Mravunac M, Hendriks JH, Verbeek AL, et al. The presence of an extensive intraductal component following a limited excision correlates with prominent residual disease in the remainder of the breast. J Clin Oncol 1990;8:113-8. 19. Veronesi U, Volterrani F, Luini A, Saccozzi R, Del Vecchio M, Zucali R, et al. Quadrantectomy versus lumpectomy for small size breast cancer. Eur J Cancer 1990;26:671-3. 20. Ghossein NA, Alpert S, Barba J, Pressman P, Stacey P, Lorenz E, et al. Importance of adequate surgical excision prior to radiotherapy in the local control of breast cancer in patients treated conservatively. Arch Surg 1992;127:411-5. 21. Gage I, Schnitt SJ, Nixon AJ, Silver B, Recht A, Troyan SL, et al. Pathologic margin involvement and the risk of recurrence in patients treated with breast conservation therapy. Cancer 1996;78:1921-8. 22. Smitt MC, Nowels KW, Zdeblick MJ, Jeffrey S, Carlson RW, Stockdale FE, et al. The importance of the lumpectomy surgical margin status in long term results of breast conservation. Cancer 1995;76;259-67. 23. Cowen D, Jacquemier J, Houvenaeghel G, Viens P, Puig B, Bardou VJ, et al. Local and distant recurrences after conservative management of "very low-risk" breast cancer are dependent events: a 10-year follow-up. Int J Radiat Oncol Biol Phys 1998;41:801-7. 24. Fisher B, Brown A, Mamounas E, Wieand S, Robidoux A, Margolese RG, et al. Effect of preoperative chemotherapy on locoregional disease in women with operable breast cancer: Findings from National Surgical Adjuvant Breast and Bowel Project B-18. J Clin Oncol 1997;15:2483-93. 25. Schnitt SJ, Harris JR, Smith BL. Developing a prognostic index for ductal carcinoma in situ of the breast. Are we there yet? Cancer 1996;77:2189-92. 26. Julien JP, Bijker N, Fentiman IS, et al. Radiotherapy in breast conserving treatment for ductal carcinoma in situ: first results of the EORTC randomised phase III trial 10853. Lancet 2000;3555: 528-33. 27. Wolmark N, Dignan J, Fisher B. The addition of tamoxifen to lumpectomy and radiotherapy in the treatment of ductal carcinoma in situ (DCIS): Preliminary results of NSABP protocol B-24. Breast Cancer Res Treat 1998;50:227. 28. McMasters KM, Giuliano AE, Ross MI, Reintgen DS, Hunt KK, Byrd DR, et al. Sentinel lymph-node biopsy for breast cancer - not yet the standard of care. New Engl J Med 1998;339:990-5. 29. Veronesi U, Paganelli G, Viale G, Galimberti V, Luini A, Zurrida S, et al. Sentinel lymph node biopsy and axillary dissection in breast cancer: results in a large series. J Natl Cancer Inst 1999;91:368-73. 30. Orr RK, Hoehn JL, Col NF. The learning curve for sentinel node biopsy in breast cancer: practical considerations: Arch Surg 1999;134:764-7. 31. Badwe RA, Mittra I. Sentinel node biopsy in breast cancer. Lancet 2001;357:2054. 32. Chetty U, Jack W, Prescott RJ, Tyler C, Rodger A. Management
of axilla in operable breast cancer treated by breast conservation:
a randomized clinical trial. Br J Surg 2000;87:163-9. 34. Orr RK. The impact of prophylactic axillary node dissection on breast cancer survival: a Bayesian meta-analysis. Ann Surg Oncol 1999;6:109-16. 35. Litwin MS, Lubeck DP, Henning JM, Carroll PR. Differences in urologist and patient assessment of health related quality of life in men with prostate cancer: results of the CaPSURE database. J Urol 1998;159:1988-92. 36. Fisher B, Bryant J, Wolmark N, Mamounas E, Brown A, Fisher ER, et al. Effect of preoperative chemotherapy on the outcome of women with operable breast cancer. J Clin Oncol 1998;16: 2672-85. 37. Vrieling C, Collette L, Fourquet A, Hoogenraad WJ, Horiot JC, Jager JJ, et al. Cosmetic assessment after breast conserving therapy in the EORTC boost versus no boost trial. Int J Radiation Oncology Biol Phys 1999;45:667-76. 38. Magee B, Swindell R, Harris M, Banerjee SS. Prognostic factors for breast recurrence after conservative breast surgery and radiotherapy: results from a randomized trial. Radiother Oncol 1996;39:223-7. 39. Riberio GG, Dunn G, Swindell R, Harris M, Banerjee SS. Conservation of breast using two different radiotherapy techniques: interim report of a clinical trial. Clin Oncol 1990;2:27-34. 40. Kuske RR, Bolton JS, et al. Brachytherapy as the sole method of breast irradiation in Tis, T1,T2, N0-1 breast cancer. Int J Radiat Oncol Biol Phys 1994;30(S1):245. © 2003 Indian Journal of Surgery. Also available online at http://www.indianjsurg.com
The following images related to this document are available:Photo images[is03066t4.jpg] [is03066t1.jpg] [is03066f1.jpg] [is03066t8.jpg] [is03066t3.jpg] [is03066t10.jpg] [is03066f2.jpg] [is03066t13.jpg] [is03066t9.jpg] [is03066t6.jpg] [is03066t11.jpg] [is03066t2.jpg] [is03066t7.jpg] [is03066t5.jpg] [is03066t12.jpg] | ||
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}