 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 65, No. 4, July-Aug, 2003, pp. 347-353 Review Article Current options in the diagnosis and management of periampullary carcinoma P. Jagannath, Shailesh Shrikhande* Department of Surgical Oncology, Lilavati Hospital, Bandra, Mumbai 400050 and *Gastrointestinal Surgical Services, Department
of Surgical Oncology, Tata Memorial Hospital, Mumbai 400012.
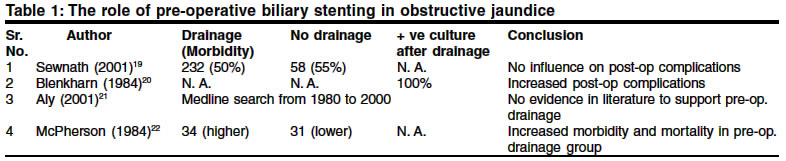
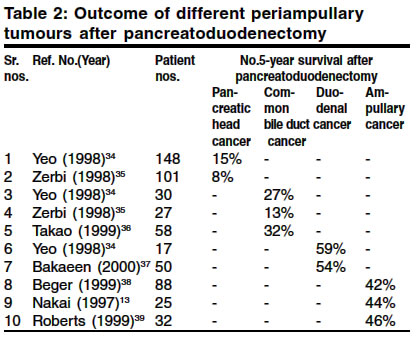
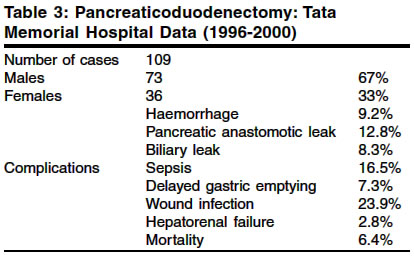
How to cite this article: Jagannath P, Shrikhande S. Current options in the diagnosis and management of periampullary carcinoma. Indian J Surg 2003;65:347-53. Paper Received: January 2002. Paper Accepted: November 2002. Source of Support: Nil Code Number: is03069 Abstract Periampullary cancers constitute a distinct entity compared to the classical pancreatic head cancer. Their diagnosis and the approach to their treatment has improved considerably in the last two decades. Endoscopy, high-resolution imaging, and endosonography have resulted in improved diagnosis and staging. A pancreatoduodenectomy offers the only chance of cure and improves survival. Superior results are seen with high volume centres. While endoscopy plays an invaluable role in the palliation of obstructive jaundice in unresectable lesions, its role in preoperative stenting remains uncertain. Adjuvant treatment modalities have so far failed to significantly improve survival. These tumours carry a better prognosis than the more dismal pancreatic head cancer, possibly because of the activation of different molecular pathways in the process of carcinogenesis. This article reviews the current understanding and various treatment options of periampullary carcinomas other than the classical pancreatic head cancer. Key Words: Periampullary tumours, Pancreatoduodenectomy, Obstructive jaundice, Ampulla of vater, Bile duct. Introduction Periampullary tumours are defined as those that arise within 2 cm of the major papilla in the duodenum. They encompass tumours of the ampulla of Vater, the distal common bile duct (intrapancreatic distal common bile duct), duodenal tumours (usually the second part) involving the papilla and tumours of the pancreatic head involving the ampulla.1 Thus, these tumours are classified on the basis of their tissue of origin. They constitute a separate entity from the classical adenocarcinoma of the pancreatic head. While these tumours can be benign, they are most commonly malignant and periampullary adenomas are well-known premalignant lesions.2 Periampullary adenocarcinomas carry a better prognosis than adenocarcinoma of the pancreatic head. While these tumours have different origins, the complex regional anatomy dictates a common operative approach. Malignant periampullary tumours are best treated by a pancreatoduodenectomy. Resection is the only option that improves survival. This review article discusses the current understanding about periampullary carcinomas, other than the classical pancreatic head cancer, and the various treatment options. History and clinical findings Periampullary tumours, compared to others in the vicinity, are diagnosed and possibly detected early on account of their anatomical location. However, there is a lack of adequate data to support this hypothesis. Though fluctuant jaundice is supposed to be typical of periampullary carcinoma, it is progressive jaundice that is more common. Thus the main feature is painless progressive jaundice in 80% of the cases; however, around 20 % cases experience fluctuating jaundice a feature unique to malignant periampullary tumours that are known to slough off.3 Patients also report significant weight loss. Abdominal pain is seen in advanced stages of the disease. In contrast, in patients with classical pancreatic head cancer, the constitutional symptoms of abdominal pain, anaemia, vomiting and weight loss usually precede jaundice. Small neuroendocrine tumours, villous adenomas and adenocarcinomas can either cause a continuous obstruction or an intermittent obstruction by a ball-valve mechanism thereby causing upper quadrant pain, jaundice and recurrent attacks of pancreatitis.4 Icterus, evidence of scratch marks all over the body due to pruritus, hepatomegaly and a palpable gall bladder are among the prominent clinical features. Molecular biology Modern molecular biology techniques have enabled investigators to search for markers in periampullary cancers. The K-ras oncogene is expressed in more than 80 % of pancreatic cancers.5 It has been shown that K-ras mutations at codon 12 are specific to pancreatic cancers and none of the other tumours in the vicinity have demonstrated this alteration. On the other hand, ampullary cancers had mutations at codon 13. These data strongly suggest that K-ras gene mutations might play a role in the pathogenesis of pancreatic cancer. Since periampullary and pancreatic cancers have different patterns of survival, Friess et al6 compared some biomolecular features of epidermal growth factor receptor (EGFR), c-erbB2, and c-erbB3. Enhanced expression of these proteins results in malignant transformation. When periampullary tumour tissues were compared with normal pancreatic tissues, no differences in expression were observed. In contrast, pancreatic cancer tissues had enhanced expression of these proteins. These findings do suggest activation of different molecular pathways in the development of ampullary and pancreatic cancers. The lack of upregulation of these factors in periampullary lesions possibly accounts for their less aggressive behaviour. A study by Bourgeois et al revealed two morphonuclear variables (related to nuclear chromatin distribution) discriminating between dysplasia and well-differentiated cancers. Furthermore, aneuploidy occurrence was associated with the discrimination between well-differentiated and poorly differentiated cancers. Thus DNA ploidy levels are expected to assist in better diagnosis of periampullary tumours.7 Another important development has been the recent demonstration that telomerase activity is common in periampullary carcinomas. The magnitude of activity correlates with aggressiveness in different periampullary carcinomas and may prove useful as a molecular index for biological staging.8 Pathology These tumours include adenocarcinomas, adenomas, tubulovillous adenomas, and villous adenomas. They are commonly sessile. Quite commonly, the preoperative clinical findings and imaging studies and even the intraoperative findings do not permit identification of the specific site of origin of a periampullary tumour. Pathological examination of resected specimens suggests that pancreatic head tumours account for 60%, while tumours of the ampulla of Vater, the distal common bile duct and duodenal tumours constitute 20%, 10% and 10% of neoplasms respectively. The majority of malignant periampullary tumours are adenocarcinomas with moderate grade histopathology. Periampullary adenomas are known to be premalignant lesions.9,10 The frequency of malignancy in adenomas is around 25 %.11 Regardless of origin, polypoid and papillary cancers have been associated with a better prognosis. Similarly, high-grade histopathology is associated with poorer prognosis compared to well-differentiated lesions. Pathological factors influencing survival in periampullary tumours Lymphatic spread While pancreatic cancers present with lymph node metastasis in 56-79% patients,12,13 periampullary tumours are associated with a 30-50% incidence of lymph node metastasis.14 Thus periampullary tumours often have limited nodal involvement compared to pancreatic cancer. Perineural invasion Perineural invasion is an important feature and usually denotes a poor prognosis. While perineural invasion is present in nearly all pancreatic cancers,15 it is noted in only 5-17 % patients with ampullary cancers.16 Investigations Biochemistry Liver functions present a typical picture of obstructive jaundice with raised direct bilirubin over indirect bilirubin and a raised alkaline phosphatase. The prothrombin time is often prolonged. Since ampullary stenosis is never complete, pancreatic function is usually normal and well preserved. No specific tumour markers are available to date. Imaging An abdominal ultrasound is an ideal preliminary test. It reveals a dilated common bile duct that can be traced right up to the ampulla with dilatation of intra-hepatic biliary radicles. It may also show an associated main pancreatic ductal dilatation and can identify the presence of possible metastatic disease in the liver, surrounding lymph nodes and ascites. A spiral CT scan can better delineate features associated with the tumour. Locoregional spread and vascular involvement can be evaluated well and its sensitivity for irresectability is around 90%.17 A contrast enhanced CT scan is therefore invaluable in the preoperative work-up of the patient. Magnetic resonance cholangiopancreatography (MRCP) has largely replaced the invasive diagnostic ERCP in delineating the cause of obstructive jaundice a common presenting feature of periampullary tumours. It provides excellent images where a clear delineation of the dilatation of the common bile duct and the intra-hepatic biliary radicles is possible. It also gives a precise idea of the status of the main pancreatic duct. A dilated main pancreatic duct right up to the ampulla differentiates a periampullary lesion from the classical pancreatic head cancer. Furthermore, it provides useful information as regards pancreatic morphology. Endoscopic ultrasound (EUS) This is a recent innovation in the world of endoscopy. Its advantage over conventional endoscopy is its ability to provide transmural details. EUS can assess the depth of tumour invasion18 from very close quarters and helps in tumour staging. Furthermore, it can assess the involvement of peri-pancreatic lymph nodes. Also, it is extremely useful in small tumours that cannot be properly assessed by CT scan. The option of EUS-guided fine needle aspiration cytology (FNAC) and brush cytology is an added asset in selected situations. Therapeutic endoscopy Its specific role is now restricted to biliary stenting to drain the obstructed common bile duct in inoperable cases and in patients who are too old or frail to undergo major resectional surgery. It is also useful to obtain a biopsy of the ampulla for confirmation of diagnosis. Biliary stenting is often performed as a preoperative measure; however, the benefits of preoperative stenting over non-intervention are unclear.19 There is evidence to suggest that biliary stenting may be harmful where their placement inevitably contaminates the bile.20 Many surgeons do not prefer preoperative biliary stenting since it induces severe inflammatory changes around the porta hepatis thereby posing operative difficulties. Furthermore, stenting often induces ascending cholangitis possibly adversely influencing postoperative outcomes.21 Table 119-22 shows some of the data relevant to preoperative biliary drainage in obstructive jaundice. Thus, biliary stenting should be performed selectively in those who are not candidates for resection, in the presence of cholangitis, when synthetic liver functions are severely deranged, and in situations where a delay between diagnosis and treatment is anticipated. Confirmation of diagnosis Duodenoscopic biopsy has certain limitations for periampullary tumours. Some studies have reported only a 50% success rate while others have shown false negative preoperative biopsies.23, 24 With the increasing availability of endoscopic facilities and expertise, one expects the percentage of success to be much higher than the one mentioned above. A negative biopsy, in a lesion with a high suspicion of malignancy, should always be questioned. The incidence of false negatives in FNAC is high and there is also an increased risk of peritoneal seedling of tumour cells.25 FNAC is therefore not advocated for periampullary tumours. Differential diagnosis 1. Ampullary fibrosis: Repeated passage of small stones / biliary sludge with resultant inflammation and fibrosis; iatrogenic injury during common bile duct exploration. 2. Motility disorders: Muscular hyperplasia, dysfunction and dyskinesia without any evidence of ampullary fibrosis. Assessment of resectability A CT scan, especially a 3-dimensional CT angiography, can point to the involvement of the superior mesenteric vessels. However, this is not routinely recommended for periampullary tumours since vascular involvement is less common compared to the classical pancreatic head cancer. Diagnostic laparoscopy just prior to surgery can help identify tiny liver and peritoneal deposits that can often be missed on CT scan examination.26 EUS, as mentioned above, can assess the depth of tumour invasion and also give an idea about the superior mesenteric and portal veins. An exploratory laparotomy is still quite often the best option. Treatment Resectional Surgery with intent to cure The resectability rate for periampullary tumours is much higher than that for ductal pancreatic adenocarcinoma. This rate is around 80% compared to 15% or so for pancreatic head cancer.27,28 Pancreatoduodenectomy (classical or pylorus-preserving) is the procedure of choice for the whole spectrum of malignant periampullary tumours in surgically fit patients. Pylorus-preserving pancreatoduodenectomy is now increasingly considered as a standard operation for periampullary or pancreatic head cancers. It has been shown to be more physiological without compromising the degree of oncological radicality and possibly results in a better quality of life.29-31 While our preference is to perform a pancreaticogastrostomy, both pancreaticojejunostomy and pancreaticogastrostomy have given equally good results in experienced hands. In doubtful cases, the patient should be prepared for a pancreatoduodenectomy and a frozen section analysis from the tumour asked for. It should be remembered that the absence of malignancy on frozen section does not definitely rule out a malignancy. In such situations, the final decision rests with the operating surgeon. The operative mortality and morbidity of this procedure has dropped significantly in the last 15 years to less than 5% and 20-30% respectively.32-34 The 5-year survival rates after resectional surgery have progressively increased. A point to note is that superior results are from referral centers specialized in pancreatic surgery.35,36 Furthermore, there are results to suggest that selected patients considered to have unresectable periampullary tumours at previous surgery should undergo restaging and reexploration at specialized high-volume centres.37 Table 238-43 shows the outcome of surgical treatment in various periampullary tumours. It is obvious that ampullary and duodenal tumours have the greatest survival after pancreatoduodenectomy. However, the survival is intermediate for distal bile duct cancers and the least for pancreatic cancers. The results show quite clearly that multiple factors other than surgical expertise and technique influence the overall survival of different periampullary tumours. The size of the tumour (< 3 cm), regional lymph node metastasis, neural invasion, and degree of differentiation appear to influence survival following resection of periampullary tumours. The results of our series of pancreatoduodenectomy at the Tata Memorial Hospital are given in Table 3. The role of extended lymphadenectomy Since the pathological behaviour of ampullary tumours is different from that of pancreatic cancer, regional lymphadenectomy has shown survival benefits in ampullary cancers.44,45 However, a prospective, randomized study of 114 patients comparing standard and extended lymphadenectomy by Yeo et al. demonstrated that while a radical pancreatoduodenectomy could be performed with similar morbidity and mortality to standard pancreatoduodenectomy, the survival data was unclear due to insufficient numbers and hence no definite conclusion could be drawn.46 Local excision of periampullary neoplasms In 1892, Sir William Halstead performed the first local excision of an ampullary tumour.47 While local excision of ampullary adenomas can be an excellent procedure, the 5-year survival rates after local excision of malignant periampullary tumours do not match the results of pancreatoduodenectomy.48 However, it is an ideal procedure for old and frail patients with carcinoma in situ who are unlikely to withstand the more morbid pancreatodudenectomy.42,49 It can also prove to be an excellent palliative measure in locally advanced lesions. If the tumours are polypoid and papillary in appearance, the results after local excision are likely to be better than in tumours with other characteristics where tumour clearance is difficult to achieve. It is important to have clear bile duct and pancreatic duct margins for anastomosis with the duodenal mucosa. Here again the role of endosonography to assess the depth of tumour invasion can prove useful. In doubtful cases with a reasonable possibility of malignancy, the risk of recurrent tumour and missed opportunity for cure following a local excision must be weighed against the complications of a pancreatoduodenectomy. It is pertinent to note that 6-10 % of patients with T1 cancers or carcinoma-in-situ harbour loco-regional lymph node metastasis.49 Palliative strategies for periampullary cancers The aim of palliative treatment is management of pain, obstructive jaundice and gastric outlet obstruction. Palliative Surgery Palliative bilio-digestive bypass procedures are indicated for patients with unresectable disease and in those with biliary obstruction or gastric outlet obstruction or both. A choledochojejunostomy or a cholecystojejunostomy combined with a gastrojejunostomy are the procedures of choice and have provided excellent long-term results with acceptable morbidity and mortality.50 However, in those who are expected to have a prolonged survival, cholecystojejunostomy is associated with recurrent obstructive jaundice after cystic duct obstruction.51,52 Therefore, a Roux-en-Y choledochojejunostomy should be the preferred technique where the rate of recurrent obstruction is very low.51- 53 Gastric outlet obstruction develops in only 10-15% cases. Therefore the role of prophylactic gastrojejunostomy is unclear and opinion remains divided. However, a randomized trial by Lillemoe et al indicated that a prophylactic gastrojejunostomy significantly decreased the incidence of late gastric outlet obstruction. It further reported that its performance does not increase incidence of postoperative complications or extend the length of stay.54 Non-surgical treatment options These options are usually reserved for the management of pain of advanced disease and for decompression of obstructed bile ducts in patients who are unfit for any form of surgery. Pain can be controlled well with narcotic analgesics or by coeliac axis blocks.55 These normally need to be repeated every three months. Endoscopic or transhepatic stenting to decompress the bile ducts should be the procedure of choice only if palliation is considered and if facilities for repeated stenting are easily available. It appears that patients expected to have a longer survival are likely to benefit from palliative surgical bypass since it precludes the need for stent exchange which may be necessary after stent obstruction, infection or migration.56,57 However, modern metallic stents are able to overcome some of the problems associated with older generation stents. As regards cost-effectiveness, a one-time surgical procedure is possibly a better alternative than repeated stentings, especially in situations where endoscopic stenting facilities are not routinely available. Adjuvant treatment options No form of adjuvant treatment has shown a definite beneficial effect in periampullary neoplasms. Recently, concurrent 5-fluorouracil (5-FU), leucovorin (LV), dipyridamole (DPM), and mitomycin-C (MMC) combined with split-course loco-regional external beam radiotherapy (EBRT) to 50 Gy has been tried. This was followed by 4 cycles of the same chemotherapy as adjuvant therapy. Early survival analysis suggests a trend towards increased median disease-free survival (8.3 vs. 17 months), especially for patients with non-pancreatic periampullary adenocarcinoma.58 Quite often adjuvant treatment is considered postoperatively but this is based on work related to pancreatic cancer and depends on the philosophy of the treating clinician. Conclusion Periampullary neoplasms, excluding those of the pancreatic head, account for nearly 40% of cases and constitute an important subsection that can be treated with optimism compared to the more dismal pancreatic head cancer. A combination of fibreoptic endoscopy, EUS and high-resolution spiral CT scans has enhanced our diagnostic abilities, our ability to stage periampullary tumours and also to assess their resectability. Pancreatoduodenectomy (pylorus-preserving) offers the best chance of cure. Results of larger studies are awaited before extended lymphadenectomy can be incorporated in standard resection protocols. A combination of tumour size, histopathological grade, lymph nodal involvement and status of resection margins, all appear to influence the overall survival of patients undergoing pancreatoduodenectomy for periampullary cancers. Since periampullary cancers vary in outcome after potentially curative resections that are well standardized, current data suggests that tumour biology probably plays a crucial role in these differences. References 1. Rattner DW, Warshaw AL. Disorders of the duodenal ampullae. In: Zinner MJ, Schwartz SI, Ellis H, editors. Maingot's Abdominal Operations. USA: Appleton and Lange; 1997. Vol. II. pp 1755-1750. 2. Kozuka S, Isuboni M, Yamaguchi A, Hachisuka K. Adenomatous residue in cancerous papilla of Vater. Gut 1981;22:1031-4. 3. Oliai A, Koff RS. Disappearance and prolonged absence of jaundice and hyperbilirubinemia in carcinoma of ampulla of Vater. Am J Gastroenterol 1973;59:518-22. 4. Kohler H, Lankisch PG. Acute pancreatitis in pancreatic cancer. Digestion 1986;35:32-3. 5. Ebert MP, Hoffmann J, Schneider-Stock R, Kasper HU, Schultz HU, Lippert H, et al. Analysis of K-ras gene mutations in rare pancreatic and periampullary tumors. Eur J Gastroenterol Hepatol 1998;10:1025-9. 6. Friess H, Wang L, Zhu Z, Gerber R, Schroeder M, Fukuda A, et al. Growth factor receptors are differently expressed in cancers of the papilla of Vater and pancreas. Ann Surg 1999;230:767-74. 7. Hittelet AB, Yeaton P, Decaestecker C, Remmelink M, Nagy N, Cremer M, Salmon I, et al. Discrimination between dysplastic and malignant epithelium of the ampulla of vater based on quantitative image cytometric data. Anal Quant Cytol Hist 2000;22: 98-106. 8. Balcom JH 4th, Keck T, Warshaw AL, Antoniu B, Graeme-Cook F, Fernandez del Castillo C. Telomerase activity in peri-ampullary tumors correlates with aggressive malignancy. Ann Surg 2001;234:344-50. 9. Geer RJ, Brennan MF. Prognostic indicators of survival after resection of pancreatic adnocarcinoma. Am J Surg 1993;165:68-72. 10. Ryan DP, Schapiro RH, Warshaw AL. Villous tumors of the duodenum. Ann Surg 1986;203:301-6. 11. Baczako K, Buechler M, Beger HG, Kirkpatrick CJ, Haferkamp O. Morphogenous and possible precursor lesions of invasive carcinoma of ampulla of vater: epithelial dysplasia and adenoma. Hum Pathol 1985;16:305-10. 12. Delcore R, Rodriguez FJ, Forster J, Hermreck AS, Thomas JH. Significance of lymph node metastasis in patients with pancreatic cancer undergoing curative resection. Am J Surg 1996;172:463-8. 13. Nagakawa T, Kobayashi H, Ueno K, Ohta T, Kayahara M, Miyazaki I. A clinical study of lymphatic flow to the paraaortic lymph nodes in carcinoma of the head of the pancreas. Cancer 1994;73:1155-62. 14. Monson JR, Donohue JH, McEntee G, McIIrath DC, van Heerden JA, Shorter RG, Nagorney DM, Ilstrup DM. Radical resection for carcinoma of ampulla of vater. Arch Surg 1991;126:353-7. 15. Ozaki H, Kinoshita T, Kosuge T, Egawa S, Kishi K. Effectiveness of multimodality treatment of resectable pancreatic cancer. Int J Pancreatol 1990;7:195-200. 16. Nakai T, Koh K, Kawabe T, Son E, Yoshikawa H, Yasutomi M. Importance of microperineural invasion as a prognostic factor in ampullary carcinoma. Br J Surg 1997;84:1399-401. 17. Fuhrman GM, Charnangavej C, Abbruzzese JL, Cleary KR, Martin RG, Fenoglio CJ, et al. Thin section contrast-enhanced computed tomography accurately predicts the resectability of malignant pancreatic neoplasms. Am J Surg 1994;167:104-13. 18. Palazzo L, Roseau G, Gayet B, Vilgrain V, Belghiti J, Fekete F, et al. Endoscopic ultrasonography in the diagnosis and staging of pancreatic adenocarcinoma. Endoscopy 1993;25:143-50. 19. Sewnath ME, Birjmohun RS, Rauws EA, Huibregtse K, Obertop H, Gouma DJ. The effect of preoperative biliary drainage on postoperative complications after pancreaticoduodenectomy. J Am Coll Surg 2001;192:726-34. 20. Blenkharn JI, McPherson GA, Blumgart LH. Septic complications of percutaneous transhepatic drainage. Evaluation of a new closed drainage system. Am J Surg 1984;147:318-21. 21. Aly EA, Johnson CD. Pre-operative biliary drainage before resection in obstructive jaundice. Dig Surg 2001;18:84-9. 22. McPherson GA, Benjamin IS, Hodgson HJ, Bowley NB, Allison DJ, Blumgart LH. Pre-operative percutaneous transhepatic biliary drainage: the results of a controlled trial. Br J Surg 1984;71:371-5. 23. Bourgeois N, Dunham F, Verkest A, Cremer M. Endoscopic biopsies of the papilla of Vater. Surg Gynecol Obstet 1983;156:297-301. 24. Leese T, Neoptolemos JP, West KP, Talbot JC, Carr-Locke DL. Tumors and pseudotumors of the region of the ampulla: an endoscopic, clinical and pathological study. Gut 1986;27:1186-92. 25. Warshaw AL. Implications of peritoneal cytology for staging of early pancreatic cancer. Am J Surg 1991;161:26-30. 26. Warshaw AL, Zhuo-yun GV, Wittenberg J, Waltman A. Preoperative staging and assessment of resectability of pancreatic cancer. Arch Surg 1990;125:230-3. 27. Ihse I, Andren-Sandberg A, Permert J, Larrson J. Early results of subtotal pancreatectomy for cancer: An interim report. In: Beger HG, Buchler MW, Malfertheiner P, editors. Standards in Pancreatic Surgery. Berlin: Springer Verlag;1993. pp. 641-5. 28. Ihse I, Larsson J. Periampullary lesions. In: Preece PE, Cushieri A, Rosin RD, editors. Cancer of the Bile Duct and the Pancreas. London: WB Saunders; 1989. pp. 83-91. 29. Yamaguchi K, Kishinaka M, Nagai E, Nakano K, Ohtsuka T, Chijiwa K, et al. Pancreatoduodenectomy for pancreatic head carcinoma with or without pylorus preservation. Hepatogastroenterology 2001;48:1479-85. 30. Seiler CA, Wagner M, Sadowski C, Kulli C, Buchler MW. Randomized prospective trial of pylorus-preserving vs. Classic duodenopancreatectomy (Whipple procedure): initial clinical results. J Gastrointest Surg 2000;4:443-52. 31. Ohtsuka T, Yamaguchi K, Chijiiwa K, Kinukawa N, Tanaka M. Quality of life after pylorus-preserving pancreatoduodenectomy. Am J Surg 2001;182:230-6. 32. Grace A, Pitt HA, Tompkins RK, DenBesten L, Longmire WP. Decreased morbidity and mortality after pancreatoduodenectomy. Am J Surg 1986;151:141-9. 33. Pellegrini CA, Heck CF, Raper S, Way LW. An analysis of the reduced morbidity and mortality rates after pancreaticoduodenectomy. Arch Surg 1989;124:778-81. 34. Rios G, Conrad A, Cole D, Adams D, Leveen M, O'Brien P, et al. Trends in indications and outcomes in the Whipple procedure over a 40-year period. Am Surg 1999;65:889-93. 35. Yeo CJ, Cameron JL, Sohn TA, Lillemoe KD, Pitt HA, Talamini MA, et al. Six hundred fifty consecutive pancreaticoduodenectomies in the 1990s: pathology, complications, and outcomes. Ann Surg 1997;226:248-57. 36. Buchler MW, Friess H, Wagner M, Kulli C, Wagener VZ, Graggen K. Pancreatic fistula after pancreatic head resection. Br J Surg 2000;87:883-9. 37. Sohn TA, Lillemoe KD, Cameron JL, Pitt HA, Huang JJ, Hruban RH, et al. Reexploration for periampullary carcinoma: resectability, perioperative results, pathology, and long-term outcome. Ann Surg 1999;229:393-400. 38. Yeo CJ, Sohn TA, Cameron JL, Hruban RH, Lillemoe KD, Pitt HA. Periampullary adenocarcinoma: Analysis of 5-year survivors. Ann Surg 1998;227:821-31. 39. Zerbi A, Balzano G, Leone BE, Angeli E, Veronesi P, DiCarlo V. Clinical presentation, diagnosis and survival of resected distal bile duct cancer. Dig Surg 1998;15:410-6. 40. Takao S, Shinchi H, Uchikura K, Kubo M, Aikou T. Liver metastasis after curative resection in patients with distal bile duct cancer. Br J Surg 1999;86:327-31. 41. Bakaeen FG, Murr MM, Sarr MG, Thompson GB, Farnell MB, Nagorney DM, et al. What prognostic factors are important in duodenal adenocarcinoma? Arch Surg 2000;135:635-41. 42. Beger HG, Trietschke F, Gansauge F, Harada N, Hiki N, Mattfeldt T. Tumor of the ampulla of vater. Arch Surg 1999;134:526-32. 43. Roberts RH, Krige JEJ, Bornman PC, Terblanche J. Pancreatoduodenectomy for ampullary carcinoma. Am Surg 1999;65:1043-8. 44. Shirai Y, Ohtani T, Tsukuda K, Hatakeyama K. Patterns of lymphatic spread of carcinoma of the ampulla of vater. Br J Surg 1997;84:1012-6. 45. Shirai Y, Tsukuda K, Ohtani T. Carcinoma of ampulla of vater. Is radical lymphadenectomy beneficial to patients with nodal disease? J Surg Oncol 1996;61:190-4. 46. Yeo CJ, Cameron JL, Sohn TA, Coleman J, Sauter PK, Hruban RH, et al. Pancreaticoduodenectomy with or without extended retroperitoneal lymphadenectomy for periampullary adenocarcinoma: Comparison of morbidity and mortality and short term outcome. Ann Surg 1999;229:613-22. 47. Halsted WS. Contributions to the surgery of the bile passages, especially the common bile duct. Boston Med Surg 1899;141:641. 48. Farnell M, Sakorafas GH, Sarr MG, Rowland CM, Tsiotos GG, Farley DR, et al. Villous tumors of the duodenum:Reappraisal of local versus extended resection. J Gastrointest Surg 2000;4:13-21. 49. Klein P, Reingruber B, Kastl S, Dworak O, Hohenberger W. Is local excision of pT1-ampullary carcinomas justified? Eur J Oncol 1996;22:366-71. 50. Sohn TA, Lillemoe KD, Cameron JL, Huang JJ, Pitt HA, Yeo CJ. Surgical palliation of unresectable periampullary adenocarcinoma in the 1990s. J Am Coll Surg 1999;188:658-69. 51. Potts JR., Brougham T, Hermann RE. Palliative operations for pancreatic carcinoma. Ann Surg 1990;159:72-7. 52. Singh SM, Longmire WP, Reber HA. Surgical palliation for pancreatic cancer. The UCLA experience. Ann Surg 1990;212:132-9. 53. Deziel DJ, Wilhelmi B, Staren ED, Doolas A. Surgical palliation for ductal adenocarcinoma of the pancreas. Am Surg 1996;62:582-8. 54. Lillemoe KD, Cameron JL, Hardacre JM, Sohn TA, Sauter PK, Coleman J, et al. Is prophylactic gastrojejunostomy indicated for unresectable periampullary cancer? A prospective randomized trial. Ann Surg 1999;230:322-30. 55. Bengtsson M, Loffstrom JB. Nerve block in pancreatic pain. Acta Chir Scand 1990;156:285-91. 56. Shephard H, Royle G, Ross A, Diba A, Arthur M, Colin Jones D. Endoscopic biliary endoprosthesis in the palliation of malignant obstruction of the distal common bile duct: a randomized trial. Br J Surg 1988;75:1166-8. 57. Smith AC, Dowsett JF, Russell RC, Hatfield AR, Cotton PB. Randomized trial of endoscopic stenting versus surgical bypass in malignant low bile duct obstruction. Lancet 1994;344:1655-60. 58. Chakravarthy A, Abrams RA, Yeo CJ, Korman LT, Donehower RC, Hruban RH, et al. Intensified adjuvant combined modality therapy for resected periampullary adenocarcinoma: acceptable toxicity and suggestion of improved 1-year disease-free survival. Int J Radiat Oncol Biol Phys 2000;48:1089-96. © 2003 Indian Journal of Surgery. Also available online at http://www.indianjsurg.com The following images related to this document are available:Photo images[is03069t3.jpg] [is03069t1.jpg] [is03069t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}