Code Number: is03070
Abstract
Though primary malignant bone tumours form only about 1% of all cancers, their aggressive natural history
makes disease control very difficult. Effective chemotherapy has improved survival and advances in imaging,
engineering and surgical techniques have made limb salvage feasible and the world has moved from amputation to limb
salvage in the majority of cases with non-metastatic disease at presentation. Indigenously developed technology
and chemotherapy protocols have allowed our own results to be comparable to those reported in the Western
literature. Newer biomaterials and fabrication methods have allowed us to develop indigenously a high-quality yet
affordable customized megaprosthesis which forms the backbone of limb salvage surgery. This paper broadly reviews
the literature and presents our own experience with the current limb salvage methods as carried out at the Tata
Memorial Hospital.
Key words: Limb salvage, Endoprosthesis, Megaprosthesis, Rotationplasty, Osteosarcoma, Ewing's sarcoma,
Biopsy, Neoadjuvant chemotherapy.
Introduction
Bone cancers are rare and form only about 1% of
the cancer load at the Tata Memorial Hospital.
These tumours have long been known to be very
aggressive in their natural history and therefore for a very
long time amputation was considered to be the only way
to achieve local control of the tumour in the limb.
Even after an amputation, only
10-20%survived,1,2 the rest succumbing to systemic
disease.3,4
In the last 30 years a sea change has occurred in
the outlook for these cancers. Chemotherapy has
allowed better local and systemic
control.5,6 Better imaging like CT and MRI have allowed the surgeon to
accurately define the extent and therefore plan tumour
resection. Advances in bioengineering have provided
exciting options for reconstruction and the world has
moved from amputation to limb salvage. In
osteosarcoma, survival improved from a dismal 10-20% to
50-70%.7,8 Long-term studies showed that limb salvage operations, performed with wide margins
and chemotherapy did not compromise the survival or
local control compared to an amputation.9-14
Though all these exciting developments occurred
in the west, in our own country, limb salvage was still
a difficult proposition. Chemotherapeutic drugs
were very expensive, endoprosthesis unaffordable, ignorance widespread and the patients poor. In
the last decade cheaper yet equally effective chemotherapeutic regimens have been
developed, bioengineering has developed indigenously and
limb salvage has become a standard method of
treatment at many centres. In this article we attempt to
present our protocols and methods in the management of
these challenging neoplasms.
Incidence
Approximately 200 new cases of primary
malignant bone tumours present to the Tata Memorial Hospital every year. Osteosarcoma is the commonest
primary bone tumour (approx 100 new cases every
year) followed by chondrosarcoma and Ewing's
sarcoma. 70% of primary bone tumours occur around the knee.
Evaluation
The patient is first assessed clinically and a
mental impression formed whether the limb is
salvageable, borderline or non-salvageable. All patients undergo
an imaging work-up for local extent and distant
spread. For suspected malignant tumours which are
clinically borderline or salvageable, an MRI of the local area
helps further define the extent and relationships to
vital structures like the neurovascular bundle. The MRI
helps to plan the margins of resection. The commonest
site of distant metastases is the chest. An X-ray chest
and where limb salvage is considered, a CT scan of the
chest (if the X-ray is clear) helps to screen for
pulmonary metastases. A bone scan is used to screen for
skips and osseous metastases. Presence of distant
metastases is generally indicative of a poor prognosis.
Biopsy
Irrespective of how typical the imaging appearance,
a histopathological diagnosis is a vital step in
the diagnostic work-up of bone tumours. Fine
needle aspiration provides only cytological material and is
not the preferred method for the diagnosis of primary
bone tumours.15 For bone tumours, the cellular
architecture as well as the quality of matrix has to be studied for
a proper diagnosis which FNAC cannot provide. A
tissue sample may be obtained either by an open
incisional biopsy or a closed core biopsy. A
sub-optimally performed biopsy may not only fail to provide
a diagnosis but may also compromise limb salvage
and even have a negative impact on overall
survival.16-21 Open biopsy, commonly performed in the past,
results in significant contamination of the surrounding
soft tissues with tumour cells. It also carries a
significant risk of infection as well as causing a
pathological fracture. Percutaneous core biopsy of bone
lesions provides early and definitive diagnosis and
guides decisions on management. The biopsy should
be performed in accordance with planned subsequent surgery.
The biopsy site chosen should be such that the
tract can be excised en bloc with the tumour. The
periphery of the tumour is the best site and the pre-biopsy
MRI may help in localizing the most representative
area. Necrotic or heavily calcified or ossified areas are avoided. In primary bone tumours, the soft tissue
mass is adequately representative for a biopsy.
Where necessary, an imaging C-arm or CT guidance is
used. We have got representative tissue in more than
90% of the cases and an error in diagnosis was found in
less than 5% of the cases.
Indications for Limb Salvage Surgery
Long-term clinical case studies have shown that a
limb salvage procedure has the same survival as an
amputation.9-14 Therefore, every patient with
a malignant tumour of the extremity is considered
for limb salvage if the tumour can be removed with
an adequate margin and the resulting limb has
satisfactory function. An adequate margin is one that results in
an acceptably low rate of local recurrence of the
tumour. An adequate margin is generally wide in most areas.
It may be close in some areas, for example in the case
of a distal femur resection, the popliteal vessels may
be on the pseudocapsule but can be easily separated
and experience has shown an acceptable low rate of
local recurrence. After salvage the limb should have
an acceptable degree of function and cosmetic
appearance with a minimal amount of pain, and should be
capable of withstanding the demands of normal daily
activities. It must look and function comparable or better than
an artificial limb after amputation. Balancing
these sometimes conflicting requirements is what makes
limb salvage surgery a complex and difficult, but
rewarding process.
In selected cases, limb salvage can be combined
with metastasectomy. For patients with
uncontrollable disease, limb salvage should be considered if
the surgery can be accomplished with minimum
morbidity and rapid return to function. These patients can
enjoy relief from pain, improved quality of life, and the
intact body image that limb salvage can offer, even if
they may not survive long.
Barriers to limb salvage
Barriers to limb salvage include poorly placed
biopsy incisions, major vascular involvement, encasement
of a major motor nerve, pathological fracture of
the involved bone, infection and inadequate motors
after resection. These adverse factors are barriers but
not absolute contraindications. For example in
pathological fractures, the fracture often heals with
chemotherapy and the specimen can be removed with
adequate margins. The ability to transfer motors, graft nerves
and vessels and provide skin cover with microsurgical methods has allowed successful limb salvage
despite many barriers. In our country, the inability to
afford chemotherapy is a major barrier to salvage.
Without cover of chemotherapy the local recurrence rate
is higher22 and therefore amputation may give the
best chance for survival.
Surgical resections and reconstruction
An adequate wide margin is a must for most
sarcomas. For bone 3 cm away from the extent on T1-MRI
image is adequate.23-28 The marrow is always sent from
the cut end for frozen section evaluation for tumour.
For the soft tissue 1-2 cm margin is preferred
wherever possible. In practice, the line between a wide and
a marginal margin is sometimes difficult to define as
the surgeon strives to control the tumour while still
leaving the patient with a useful limb. However, when in
doubt, the surgeon errs on the side of excess tissue
removal. The adequacy of the margin can be judged by
bivalving the specimen. If there is any doubt about margins
a decision for an amputation can be made on table.
This is the reason that any patient undergoing a limb
salvage procedure is forewarned about this possibility
and consent for amputation always obtained.
After completion of the tumour resection, the
surgeon must reconstruct the resulting surgical defect.
The surgeon must eliminate potential deadspace and transfer tissues if necessary to allow an
effective closure. Most bone sarcomas occur in the
metaphyseal portion of the bone, so that typical resection
involves the whole proximal or distal part of the bone.
The gap remaining needs reconstruction either with
metal or with bone or a composite of the two. Endoprosthesis is the most common method used
as it provides immediate stability and mobility
without interfering with any adjuvant treatment. An
imported prosthesis, though of excellent quality, is
very expensive (price Rs 3.5 lacs) and out of reach of
most of our patients. We have therefore developed
an indigenous stainless steel prosthesis at 10% of the cost of the imported joint. This joint has now
been used in over 80 cases with excellent
short-term results. We have also developed shoulder, hip
and elbow megaprostheses. Recently, we have
developed and used even total humerus, total femur and
saddle pelvic prosthesis. The latter was used to
reconstruct the defect after internal hemipelvectomy.
For tumours that involve the diaphyseal portion of
a bone, an intercalary resection and reconstruction
can be performed that saves the joints at either end.
Small resected segments of bone are reconstructed
using autogenous bone from the patient's iliac crest or
other sites, but the available supply is strictly limited. In
most cases the excised segment of bone must be
replaced, either by a large internal prosthesis, a segment
of allograft bone, a composite of an allograft and
a prosthesis, or by other methods. The tissue bank at
the Tata Memorial Hospital provides freeze- dried
irradiated long segment allografts which we have used
to reconstruct intercalary defects with good success.
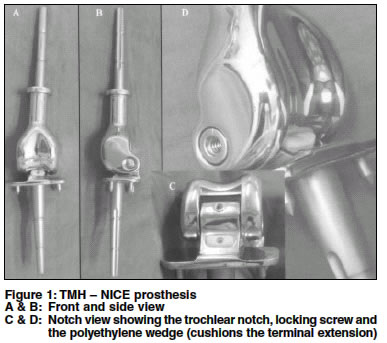
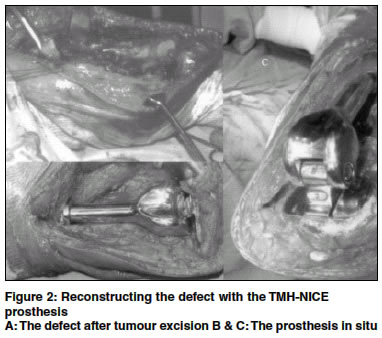
At the Tata Memorial Hospital, the authors
have designed and standardized a low-cost
customized prosthesis called Tata Memorial Hospital
New Indigenous Custmozed Endoprosthesis (TMH-NICE) (Figures 1 & 2). This prosthesis has been used in
over 30 patients over the last 18 months with excellent
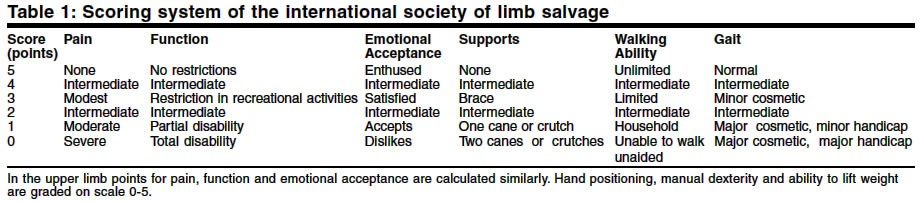
early results (Figure 3). The functional score as assessed
by the modified Enneking system (Table 1) We had
an average score of 24 out of posssible 30
corresponding to 80% function score.
Osteosarcoma - guidelines
Osteosarcoma is the commonest primary
malignant bone tumour. Approximately 100 cases present to
our hospital every year. Almost 50% present with metastatic disease or with locally advanced
disease. The prognosis is poor with metastatic disease.
The commonest age is between 12-25 yrs with males outnumbering the females. The distal femur is
the commonest site followed by the proximal tibia.
Figure 4 shows the case of a 19-year old male treated
with NICE prosthesis.
Preoperative chemotherapy
Once tissue diagnosis is made, chemotherapy
is advised. This chemotherapy is given as per the established hospital protocols. Anterior
chemotherapy is given for the following reasons:
- It controls micrometastases and
improves survival5,6
- It allows time for the fabrication of a customized endoprosthesis
- The response to chemotherapy can be
evaluated after surgery. This is the single most
important prognostic factor29-31
- A good response to chemotherapy makes
limb salvage surgery easier by:
- Decrease in tumour size and vascularity
- Pseudocapsule becomes thick and composed
of mature fibrous tissue and finger-like
projections of the tumour through the
pseudocapsule disappear22
- Decrease in local recurrence
rate22
The best chemotherapy results came initially from
high dose methotrexate-based
regimens.5-7,32 However, these regimens were expensive and toxic and a shift
is occurring towards protocols without
methotrexate.33-37 Adriamycin, cisplatinum, ifosfamide and etoposide
are the effective drugs against osteosarcoma.
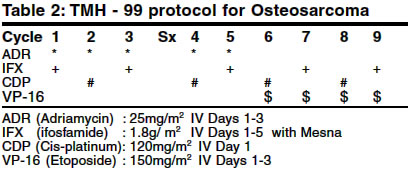
At the Tata Memorial Hospital, we are using a
non-methotrexate-based chemotherapy protocol (Table
2). Adriamycin is given alternating with ifosfamide
and cisplatinum for five cycles. Surgery is done after
5 cycles. After this adriamycin is replaced with
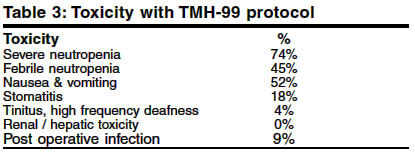
etoposide for the next 4 cycles. Chemotherapy has to be
given under expert supervision as toxicity is substantial
(Table 3). Inadequate care during febrile neutropenia
or cardiotoxicity can result in fatality. We have had
two deaths related to chemotherapy toxicity.
Fortunately, these patients are young with no systemic
compromise and tolerate the chemotherapy well. The cost
of chemotherapy is still high and many of our
patients are unable to afford it.
3 to 5 cycles are given prior to surgery. During
this time the customized joint is ordered. If metastases
are present they are reevaluated after
chemotherapy. Metastatectomy can be combined with limb
salvage surgery in selected cases.
After surgery the specimen is sent for evaluation
of chemotherapy response. It is cut into multiple
sections, and each analyzed for percentage of necrosis.
The pathologist then averages all sections to give
the response in terms of percentage tumour necrosis.
We use Huvos' grading 36 (Table
4 ).
The single best prognostic factor following preoperative chemotherapy has been > 90%
necroses.29,37,38 For those with complete response (100% necrosis),
10-year survival is estimated to be
90%.30 In our series we have approximately 70% patients showing a
good response to chemotherapy.
Following surgery, chemotherapy is started after
suture removal. Patient is followed up periodically with
CT scans. The commonest site of disease recurrence is
the lung (70-80%) followed by the bone (15-20%). The
local recurrence rate is around 5-10% for the limbs. 89%
of the recurrences occur within 18 months of
diagnosis.22
Ewing's family of tumours
The Ewing's family of tumours includes
Ewing's sarcoma of bone, primitive neuroectodermal
tumour (PNET) of the bone and soft tissues, and Ewing's
tumour of the soft tissues. These are all small round
cell tumours. For long, Ewing's tumours have been
known to be extremely sensitive to radiation. While
surgery or irradiation could provide local control in 50-70%
of cases,39 more than 90% eventually died of
metastatic disease.40,41 Like in osteosarcoma,
multiagent chemotherapy developed in the 70s improved
overall survival by controlling micrometastases and
reducing local failure.41-44 The role of surgery is not yet
precisely defined. Radiation had been the preferred method
of local control due to the morbidity associated
with surgery. Recent reports indicate that surgery
combined with chemotherapy and with or without radiation
may have better local control rates than chemotherapy
with radiation alone.45-51
Management of round cell tumours, therefore,
requires a team approach. All these patients are best
discussed in a joint clinic involving medical
oncologists, radiotherapists, orthopaedic surgeons and
radiologists. The feasibility of wide resection without
significant morbidity and loss of function is evaluated. The
decision is made using various imaging modalities like
plain radiographs, CT, MRI, bone scans, etc to determine
size, extent, soft tissue mass and muscle involvement
and neurological / vascular involvement.
Surgery is preferred wherever complete surgical excision is feasible without significant functional
loss like in fibula or rib. Where margins are close or
involved, radiation can be added postoperatively. The dose
can be reduced, thereby also reducing the
complications. Lesser tumour load also improves the efficacy of
the administered dose.
Irrespective of the local treatment,
multi-drug chemotherapy is always given and is the mainstay
in the management of the Ewing's family of
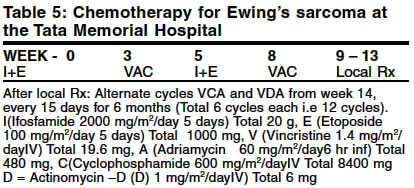
tumours. Ifosfamide, etoposide, vincristine,
adriamycin, cyclophosphamide and actinomycin-D are the
agents used in the protocol running at the Tata
Memorial Hospital (Table 5). 4 cycles of induction therapy
are used (each cycle lasts 3 weeks). After this a decision
of modality for local control is made. Like in osteosarcoma, response to chemotherapy is
an important prognostic factor.52-54 This information
is available only in the operated cases. Chemotherapy
is resumed soon after suture removal.
Complications
Massive and long surgical procedures in
patients compromised by chemotherapy or radiotherapy
make the patient prone to complications. Various complications, both intraoperative and postoperative
are seen in limb salvage surgery. Minor wound
complications like collection or haematoma or edge necrosis are
seen in 5-8%. Deep infection rate is about 5% and
can compromise the final outcome. Late infections are
a lifelong hazard with maximum risk during
postoperative chemotherapy. Intraoperative complications
include arterial injury and nerve palsies but these are quite
rare. Implant-related complications like breakage,
loosening occur over a longer period of time. Local recurrence
is seen in about 8-10% of cases and distant metastases
in about 30-40%. It is because of this propensity
to complications that the patient is forewarned
about multiple surgical procedures or even amputation.
Conclusion
The first decade of the new millennium has been
globally recognized by the orthopaedic fraternity as the
decade of improvements in the treatment of bone and
joint disorders. An ideal situation in the management of
bone tumours is when the disease can be
successfully removed without an amputation and the resulting
loss of bone and muscle is compensated by a method
which retains near normal limb function. Patient survivals
have dramatically improved following the availability
of newer chemotherapy drugs and this has accentuated the need for durable methods of reconstruction of
large musculoskeletal defects. Orthopaedic surgeons
have risen to the challenge and it is now possible to
offer limb salvage to a large majority of patients with
bone tumours. Ever-increasing advances in technology
and biomaterials combined with a better understanding
of biomechanics will further help in increasing
the durability and refining limb salvage procedures.
Though complications occur, the ultimate outcome is
highly satisfactory in the majority of cases.
Acknowledgements
The authors acknowledge the help and intellectual
input of Sushrut Surgicals in the design and fabrication of
the TMH-NICE endoprosthesis.
References
1. Dahlin DC, Coventry MB. Osteosarcoma a study of 600 cases.
J Bone Joint Surg 1967;49A:101-10.
2. Marcove RC, Mike V, Hajeh JV, Levin AG, Hutter RV.
Osteosarcoma under the age of twenty one: A review of one hundred
and forty five operative cases. J Bone Joint Surg 1970;52:411-23.
3. Huth JF, Eilber FR. Patterns of recurrence after resection of
osteosarcoma of the extremity: strategies for treatment of
metastases. Arch Surg 1989;124:122-6s.
4. Bacci G, Avella M, Picci P, Briccoli A, Dallari D, Campanacci
M. Metastatic patterns in osteosarcoma. Tumori 1988;74:421-7.
5. Link MP, Goorin AM, Miser AW, Green AA, Pratt CB, Belasco
JB, et al. The effect of adjuvant chemotherapy on relapse free
survival in patients with osteosarcoma of the extremity. New Eng
J Med 1986;314:1600-6.
6. Eilber F, Giuliano A, Eckhardt J, Patterson K, Moseley S,
Goodnight J. Adjuvant chemotherapy for osteosarcoma: a randomized
prospective trial. J Clin Oncol 1987;5:21-6.
7. Meyers PA, Heller G, Healy J, Huvos A, Lane J, Marcove R, et
al. Chemotherapy for non-metastatic osteogenic sarcoma: the
Memorial Sloan-Kettering experience J Clin Oncol 1992;10:5-15.
8. Baci G, Ferrari S, Bertoni F, Ruggieri P, Picci P, Longhi A, et
al. Long term outcome for patients with non-metastatic
osteosarcoma of the extremity treatment at the istituto ortopedico
Rizzoli according to the istituto ortopedico Rizzoli / osteosarcoma-2
protocol: an updated report. J Clin Oncol 2000;18:4016-27.
9. Sim, FH, Ivins JC, Taylor WF, Chao EYS. Limb-sparing surgery
for osteosarcoma: Mayo Clinic experience. Cancer Treat
Sympos 1985;3:139-54.
10. Lane JM, Glasser DB, Duane K, Healey JH, McCormack RR,
Rosen G, et al. Osteogenic sarcoma: two hundred thirty-three
consecutive patients treated with neoadjuvant chemotherapy.
Orthop Trans 1987;11:495.
11. Goorin AM, Perez-Atayde A, Gebhardt M, Andersen JW,
Wilkinson RH, Delorey MJ, et al. Weekly high-dose methotrexate
and doxorubicin for osteosarcoma: The Dana-Farber Cancer Institute
/ The Children's Hospital - Study III. J Clin Oncol 1987;5:1178-84.
12. Simon MA, Aschliman MA, Thomas N, Mankin HJ.
Limb-salvage treatment versus amputation for osteosarcoma of the distal
end of the femur. J Bone Joint Surg 1986;68:1331-7.
13. Winkler K, Beron G, Kotz R, Salzer-Kuntschik M, Beck J, Beck
W, et al. Neoadjuvant chemotherapy for osteogenic sarcoma.
Results of a cooperative German/Austrian Study. J Clin
Oncol 1984;2:617-24.
14. Rougraff BT, Simon MA, Kneisl JS,Greenberg DB, Mankin HJ.
Limb salvage compared with amputation for osteosarcoma of the
distal end of the femur. A long-term oncological, functional, and
quality-of-life study. J Bone Joint Surg 1994;76:649-56.
15. Van der Bijl AE, Taminiau AHM, Hermans J, Beerman
H, Hogendoorn PCW. Accuracy of the Jamshidi trocar biopsy in
the diagnosis of bone tumors. Clin Ortho Rel Res 1997;334:233-43.
16. Bickels J, Jelinek JS, Shmookler BM, Neff RS, Malawer MM.
Biopsy of musculoskeletal tumors. Clin Ortho Rel Res 1999;368:212-9.
17. Mankin HJ, Mankin CJ, Simon MA. The hazards of the
biopsy, revisited. J Bone Joint Surg 1996;78;656-63.
18. Mankin HJ, Lange TA, Spanier SS. The hazards of biopsy in
patients with malignant primary bone and soft-tissue tumors. J
Bone Joint Surg 1982;64:1121-7.
19. Enneking WF. The issue of the biopsy. J Bone Joint
Surg 1982;64:1119-20.
20. Simon MA. Current concepts review. Biopsy of
musculoskeletal tumors. J Bone Joint Surg 1982;64:1253-7.
21. Springfield DS, Rosenberg A. Biopsy: complicated and risky.
J Bone Joint Surg 1996;78:639-43.
22. Picci P, Sangiorgi L, Rougraff BT, Neff JR, Casadei R,
Campanacci M. Relationship of chemotherapy induced necrosis and
surgical margins to local recurrence in osteosarcoma. J Clin
Oncol 1994;12:2699-705.
23. Aisen AM, Martel W, Braunstein EM, McMillin KI, Phillips
WA, Kling TF. MRI and CT evaluation of primary bone and
soft-tissue tumors. Am J Roentgenol 1986;146:749-56.
24. Cohen MD, Weetman RM, Provisor AJ, Grosfeld JL, West
KW, Cory DA, et al. Efficacy of magnetic resonance imaging in
139 children with tumors. Arch Surg 1986;121:522-9.
25. Gillespy T 3rd, Manfrini M, Ruggieri P, Spanier SS, Pettersson
H, Springfield DS. Staging of intraosseous extent of
osteosarcoma: Correlation of preoperative CT and MR imaging with
pathologic macroslides. Radiology 1988;167:765-7.
26. Golfieri R, Baddeley H, Pringle JS, Leung AW, Greco A,
Souhami R. MRI in primary bone tumors: Therapeutic implications. Eur
J Radiol 1991;12:201-7.
27. O'Flanagan SJ, Stack JP, McGee HM, Dervan P, Hurson B.
Imaging of intramedullary tumour spread in osteosarcoma: A
comparison of techniques. J Bone Joint Surg 1991;73:998-1001.
28. Onikul E, Fletcher BD, Parham DM, Chen G. Accuracy of
MR imaging for estimating intraosseous extent of osteosarcoma.
Am J Roentgenol 1996;167:1211-5.
29. Goorin AM, Shuster JJ, Baker A, Horowitz ME, Meyer WH,
Link MP. Changing pattern of pulmonary metastases with
adjuvant chemotherapy in patients with osteosarcoma: results from
the multiinstitutional osteosarcoma study. J Clin Oncol 1991;9:600-5.
30. Link MP, Goorin AM, Horowitz M. Adjuvant chemotherapy of
high grade sarcoma of the extremity. Clin Orthop 1991;270:8-14.
31. Raney RB, Asmar L, Newton WA Jr, Bagwell C, Breneman JC,
Crist W, et al. Ewing's sarcoma of soft tissues in childhood: a
report from the Intergroup Rhabdomyosarcoma Study. J Clin
Oncol 1997;15:574-82.
32. Rosen G, Caparros B, Huvos AG, Kosloff C, Nirenberg A,
Cacavio A, et al. Preoperative chemotherapy for osteogenic
sarcoma. Selection of postoperative adjuvant chemotherapy based on
the response of the primary tumor to preoperative
chemotherapy. Cancer 1982;49:1221-30.
33. Souhami RL, Craft AW, Van der Eijken JW, Nooij M, Spooner D, Bramwell VH, et al. Randomised trial of two regimens of
chemotherapy in operable osteosarcoma: a study of the European
Osteosarcoma Intergroup. Lancet 1997;350:911-7.
34. Krailo M, Ertel I, Makley J, Fryer CJ, Baum E, Weetman R, et al.
A randomized study comparing high-dose methotrexate with
moderate dose methotrexate as components of adjuvant
chemotherapy in childhood nonmetastatic osteosarcoma: a report
from the Childrens Cancer Study Group. Med Pediatr
Oncol 1987;15:69-77.
35. Bramwell VH, Burgers M, Sneath R, Souhami R, van
Oosterom AT, Voute PA, et al. A comparison of two short intensive
adjuvant chemotherapy regimens in operable osteosarcoma of limbs
in children and young adults: the first study of the European
Osteosarcoma Intergroup. J Clin Oncol. 1992;10:1579-91.
36. Huvos A, Rosen G, Marcove RC. Primary osteogenic
sarcoma: pathologic aspects in 20 patients after treatment with
chemotherapy, en bloc resection and prosthetic bone replacement.
Arch Pathol Lab Med 1977;101:14.
37. Davis AM, Bell RS, Goodwin PJ. Prognostic factors in
osteosarcoma: a critical review. J Clin Oncol 1994;12:423-31.
38. Bacci G, Briccoli A, Mercuri M, Ferrari S, Bertoni F, Gasbarrini
A, et al. Osteosarcoma of the extremities with synchronous
lung metastases: long-term results in 44 patients treated
with neoadjuvant chemotherapy. J Chemother 1998;10:69-76.
39. Pizzo AA, Poplack DG. Principles and Practice of Paediatric
Oncology, 3rd edn. Lippincott Raven Publishers; 1997.
40. Dahlin DC, Coventy MD, Scanlon PW. Ewing's sarcoma: a
critical analysis of 165 cases. J Bone Joint Surg Am 1962; 43:185.
41. Wang CC, Schultz MD. Ewing's sarcoma. N Engl J
Med 1953;248:571.
42. Perez CA, Tefft M, Nesbit M, Burgert EO Jr, Vietti T, Kissane J,
et al. The role of radiation therapy in the management of
non-metastatic Ewing's sarcoma of bone: report of the Intergroup
Ewing's Sarcoma Study. Int J Radiat Oncol Biol Phys 1981;7:141-9.
43. Cangir A, Vietti TJ, Gehan EA, Burgert EO Jr, Thomas P, Tefft M,
et al. Ewing's sarcoma metastatic at diagnosis: results and
comparisons of two intergroup Ewing's sarcoma studies.
Cancer 1990;66:887-93.
44. Fernandez CH, Lindberg RD, Sutow WW, Samuels ML.
Localized Ewing's sarcoma: treatment and results. Cancer 1974;34:143-8.
45. Nesbit ME Jr, Gehan EW, Burgert EO Jr, Vietti TJ, Cangir A, Tefft
M, et al. Multimodal therapy for the management of
primary nonmetastatic Ewing's sarcoma of bone: a long-term
follow-up of the first intergroup study. J Clin Oncol 1990;8:1664-74.
46. Marcove RC, Rosen G. Radical en bloc excision of Ewing's
sarcoma. Clin Orthop 1980;153:86-91.
47. Rosen G. Primary Ewing's sarcoma: the multidisciplinary
lesion. Int J Radiat Oncol Biol Phys 1978;4:527.
48. Sailer SL, Harmon DC, Mankin HJ, Truman JT, Suit HD.
Ewing's sarcoma: surgical resection as a prognostic factor. Int J
Radiat Oncol Biol Phys 1988;15:43.
49. Conner MI, Pritchard DJ: Ewings Sarcoma. Clin Orthop Rel
Res 1991;262:78.
50. Hoffmann C, Ahrens S, Dunst J, Hillmann A, Winkelmann W,
Craft A, et al. Pelvic Ewing sarcoma: a retrospective analysis of
241 cases. Cancer 1999; 85:869-77.
51. Yaw KM: Pediatric bone tumors. Seminars Surg
Oncol 1999;16:173-83.
52. Bacci G, Ferrari S, Bertoni F, Rimondini S, Longhi A, Bacchini P,
et al. Prognostic factors in nonmetastatic Ewing's sarcoma of
bone treated with adjuvant chemotherapy: analysis of 359 patients
at the Istituto Ortopedico Rizzoli. J Clin Oncol 2000;18:4-11.
53. Rosito P, Mancini AF, Rondelli R, Abate ME, Pession A, Bedei L,
et al. Italian Cooperative Study for the treatment of children
and young adults with localized Ewing sarcoma of bone: a
preliminary report of 6 years of experience. Cancer 1999; 86:421-8.
54. Wunder JS, Paulian G, Huvos AG, Heller G, Meyers PA,
Healey JH. The histological response to chemotherapy as a predictor
of the oncological outcome of operative treatment of Ewing
sarcoma. J Bone J Surg 1998;80:1020-33.
© 2003 Indian Journal of Surgery. Also available online at http://www.indianjsurg.com


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}