 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 65, No. 4, July-Aug, 2003, pp. 361-365 Original Article Sentinel node biopsy in operable breast cancer V. Parmar, R. Badwe, I. Mittra, R. Chinoy,* R. Hawaldar** Departments of Surgical Oncology, *Pathology and **Clinical Research Secretariat, Tata Memorial Hospital, Ernest Borges Road,
Parel, Mumbai 400012, India.
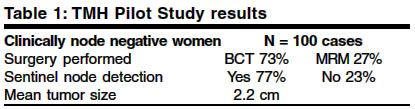
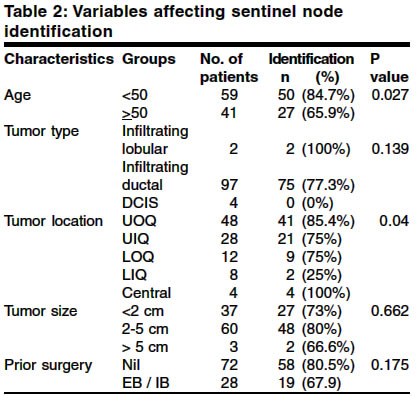
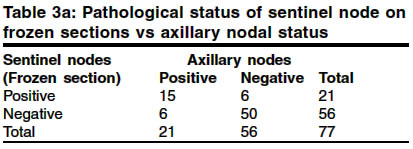
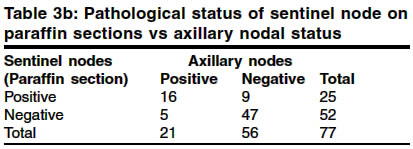
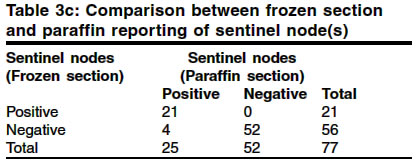
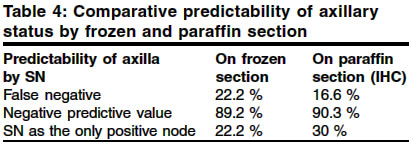
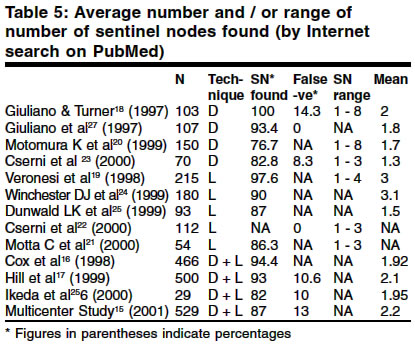
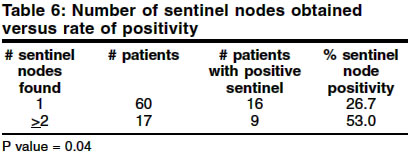
How to cite this article: Parmar V, Badwe R, Mittra I, Chinoy R, Hawaldar R. Sentinel node biopsy in operable breast cancer. Indian J Surg 2003;65:361-5. Paper Received: January 2002. Paper Accepted: June 2002. Source of Support: Nil Code Number: is03071 Abstract The advent of mammography and increased awareness about breast cancer has resulted in the detection of smaller tumours. The majority of these small tumours would not have had metastasized to the axillary lymph nodes. Sentinel node biopsy (SNB) in operable breast cancer has gained popularity since it promises to avoid treatment of the axilla when the nodes are negative for metastasis. However, it has not been able to achieve its objective. The world literature quotes a false negative rate ranging from 4.7% to 12.5% on immunohistochemistry while our own results of a pilot study at the Tata Memorial Hospital (TMH) have shown a false negative rate as high as 16.6% (22.2% on frozen section). The consequence of leaving behind untreated positive non-sentinel nodes in the axilla is a potential risk for axillary recurrence. Axillary sampling is a simple and inexpensive procedure in which level I nodes are removed by a blind dissection. We have tried to critically analyze the efficacy of both the procedures, i.e. targeted sentinel node biopsy versus blind axillary sampling to see whether the latter could be a preferred alternative in terms of accuracy and cost-effectiveness in countries with limited resources. Key Words: Sentinel node biopsy, Axillary sampling, Operable breast cancer Introduction In women with a clinically node negative operable breast cancer the incidence of nodal metastasis is approximately 30%.1 With the growing popularity of mammography and an increase in the incidence of screen-detected cancers, smaller tumours are now being detected, where the proportion of cases with nodal metastases is low. The benefits of surgical clearance of the axilla in early breast cancer are evidently restricted to node positive cases. A complete axillary clearance, with its associated morbidity,2-4 is considered over-treatment in pathologically node negative women and should be avoided if these cases could be identified in advance. The concept of sentinel node (SN) is founded on the belief that breast cancer spreads in an orderly fashion with initial spread to the first or `sentinel' node in the lymphatic basin and then to the rest of the regional lymph nodes. If the sentinel node could be identified and confirmed to have no metastasis, the assumption is that the rest of the axilla is also uninvolved. Thus, the identification of the sentinel node gained popularity with the hope to identify correctly node negative axillae so that surgery and its associated morbidity could be avoided. Per-operative sentinel node identification has been carried out using various techniques. In the visual method, the blue-stained node(s) are identified a few minutes after an intra-tumoral or peri-tumoral injection of 1% isosulphan blue dye. The other technique has been the radio-localization of the sentinel node using a hand-held gamma-probe a few hours after a local injection of radio-labelled colloid particles. Several validation studies have been carried out all over the world to find out the predictability and reliability of sentinel node biopsy (SNB) in correctly identifying the negative axilla.5 In an editorial, McMasters had published an overview of eleven studies5 of SNB in 1385 women with clinically node negative operable breast cancer in 1998. The results showed that sentinel node could be identified correctly in 86% (range 66-98%) of cases. The identification was better when blue dye and radio-labelled colloid were used in combination.6 SNB had a sensitivity of 94%, a negative predictive value of 97% and 98% accuracy in predicting the axilla. The procedure carried a false negative rate of 6.2% (range 4.7-12.5%) after immunohistochemistry5 of SN. If the decision for performing axillary clearance was to be based primarily on the SN results, the axilla would be under-treated in those women with a false negative result and they would carry a certain risk of axillary recurrence.7 The long-term consequences of leaving behind untreated metastatic nodes in the axilla, are being addressed in randomized trials of SNB vs. complete axillary clearance conducted by NSABP-B32; the Medical Research Council of the United Kingdom funded ALMANAC trial; and the ACOSOG-Z0011 trial by the American College of Surgeons, the results of which are all still awaited.8,35,36 The other important controversy is regarding the method of treatment of the sentinel node detected positive axilla, by a complete axillary dissection versus axillary irradiation alone. Modern techniques of axillary irradiation have definitely reduced the incidence of morbidity following radiotherapy to axilla. The ALMANAC (UK) trial is presently comparing axillary clearance and axillary irradiation in sentinel node-positive patients and may help resolve this issue. 35 Material and methods A sentinel node validation (pilot) study was carried out at the Breast Unit at TMH using 1% isosulphan blue dye. 100 consecutive patients with a primarily operable, clinically node-negative breast cancer were enrolled between April 1999 and Nov 2000. 3 to 4 ml of patent blue dye was injected intra-tumorally and peri-tumorally towards the axilla, and 0.5 ml was injected subdermally over the tumour. The axilla was explored after 10-15 minutes to detect any blue-stained lymph node(s). The blue node(s) was then sent for frozen section, wherein the node was sliced into two. One half was sent for routine histology and immunohistochemistry, and from the other half, two sections were processed for frozen section analysis. The axilla was completely cleared in all cases without waiting for the frozen section report. The axillary specimen was sent for final histopathological analysis. Both residents and consultants performed the procedure after a trial run in 20 cases. Results The number of patients studied and the surgeries performed are listed in Table 1. The overall incidence of nodal metastases in clinically node-negative patients in our study was 36.7%. Sentinel node could be identified in only 77% of the cases, indicating a technical failure of the procedure in 23% of cases wherein no blue node could be found. There was no significant univariate relation between finding a sentinel node and tumour size, tumour type or prior incision or excision biopsy performed. However, age 50 years or more and a primary tumour in a medial location were significantly associated with a failure to identify the sentinel node (Table 2). Sentinel nodes were detected in level I in 94.8% cases, and in level I and II in 5.2% cases. No sentinel node was found in the interpectoral tissue or in level III. The mean number of sentinel nodes found in our study was 1.4 (range 1-6). In 77.9% cases only one sentinel node was identified. The sentinel node was the only positive node in the axilla in 30%, i.e. 9 out of 30 cases. In all, 21 patients were predicted to have a positive axilla on frozen section, while 6 cases were missed in the presence of metastases in downstream lymph nodes. Frozen section assessment of the sentinel node thus yielded a high false negative rate of 22.2% (6 out of 27 cases) in predicting the axillary status. On paraffin section reporting of the sentinel nodes, 4 cases where SN had been reported negative on frozen section were upstaged by detection of micrometastases. The false negative rate after immunohistochemistry on paraffin sections of the sentinel nodes was thus 16.6%, i.e. 5 out of 30 cases (Tables 3a, b, c). The negative predictive value was 89.2% on frozen section and improved to 90.3% after paraffin section and immunohistochemistry (Table 4). Discussion Technological advances in SNB still carry a high procedural failure rate where either no sentinel nodes are identified or an incorrect prediction of a negative axilla is made. Where identified, there has also been a wide variation in the numbers of sentinel nodes removed. We carried out an Internet search in PubMed by putting in the terms `sentinel node' and `breast cancer' and came across more than 130 studies on SNB. 13 studies15-27 had a mention of either the actual numbers or mean number of sentinel nodes found in the published abstracts (Table 5). The number of nodes dissected by SNB ranged from 1 to 8 with a mean of 2.05 (range of mean 1.3-3.1). This observation poses a threat to the very hypothesis of a `first echelon' or a `sentinel node'. In a large multicentre trial15 the percentage of positive sentinel nodes was found to be higher if 2 or more sentinel nodes were removed (p=0.025) and the authors have concluded that the possibility of missing a positive non-sentinel node is higher if lesser number of sentinel nodes are dissected. The SNB study at TMH also showed that there was a statistically significant correlation between the number of sentinel nodes found and the number of pathologically positive sentinel nodes when 2 or more sentinel nodes are identified (p = 0.04) (Table 6). The possible inference from the above is that more the number of sentinel nodes identified there is a corresponding increase in sensitivity with lower false negative rates. Wong et al34 have also observed that the false negative rates were 14.3% and 4.3% for patients with a single sentinel node vs. multiple sentinel nodes removed, respectively (p=0.0004). They concluded that the ability to identify multiple sentinel nodes, when they exist, improves the diagnostic accuracy of sentinel lymph node biopsy. Krag et al observed a significant positive correlation between the number of pathologically positive sentinel nodes and the number of positive non-sentinel nodes obtained at axillary lymphadenectomy (Spearman's rank-correlation coefficient, 0.49; p<0.001) in a multicentre validation study29 of SNB in 443 patients. This clearly indicates that the sensitivity of the sentinel node procedure is directly proportional to the number of sentinel nodes dissected. Axillary sampling, a simpler technique of limited axillary intervention, was investigated in the past9-11 with the intent to identify a node-positive axilla with a less invasive procedure compared to axillary clearance and thus select candidates for axillary treatment by irradiation. The number of nodes recommended for a representative axillary sampling from level I for appropriate prediction of axillary status was four to five nodes.28 If the procedure failed to yield the number of nodes required at the first attempt, further dissection of level I nodes was carried out till the required target number of nodes sampled was achieved. Thus, the yield was 100% with no failure of procedure in comparison to sentinel node biopsy. There is a validation study of lower axillary sampling vs. total axillary clearance reported by Steele et al12 in 1985 with a sensitivity of 100% and an accuracy of 99.5%. A more recent validation study of 5-node axillary sampling compared to level I-II dissection was reported from Stockholm13 on 416 operable breast cancer patients. The noteworthy finding was that node sampling had a 100% yield, 97.3% sensitivity and a negative predictive value of 98.5%, which are obviously better figures than those reported in literature5 for sentinel node biopsy, i.e. 94% sensitivity and 97% negative predictive value. The Edinburgh sampling study30 in 799 patients observed that the percentage of node-positive patients did not increase significantly as the number of sampled positive nodes increased beyond 4. In contrast, in the sampling study conducted in the UK31, it was observed that an increase in the number of nodes harvested by sampling was associated with the detection of a higher proportion of node-positive patients and a higher number of metastatic nodes were identified. In this sampling study, a median of 8 nodes was identified (range 0-30) and in only 11 patients less than 4 nodes were identified. There is an observed learning curve for SNB with lower identification rate and higher false negatives at the beginning of the study improving with increasing experience.14,15 On the other hand, axillary node sampling has a 100% node detection rate13 and being a simple surgical technique, has no evident learning curve. Thus, axillary sampling may be a simpler and more feasible alternative to SNB in women with operable breast cancer without the necessity for (expensive) gadgetry like radio-localization gamma probes or the (messy) procedure of injection of vital blue dye. This is important especially in developing countries with limited resources, as it does not involve any additional investment.32 Axillary sampling and SNB should, however, be tested in a randomized setting to compare the resultant morbidity and false negative rates before adopting either method as standard clinical practice. The Nottingham group33 have recently published the results of a prospective study to find out the value of adding SNB to 4-node axillary sampling (4NAS) within the same patient. 200 patients were accrued and 4NAS was found to have a lower false negative rate compared to SNB. A study comparing SNB and low axillary sampling in a randomized setting is also being proposed at the Breast Unit in the Tata Memorial Hospital, Mumbai, India. The study will require to accrue 300 women with clinically node-negative operable breast cancer, 150 in each arm, at a baseline sentinel node detection rate of 87% and have 80% power and 95% CI to be able to detect an anticipated improvement rate of 10%. Acknowledgements We would like to thank the department of Clinical Research Secretariat for their valuable help in the compilation and analysis of data. References 1. Sacks NPM, Baum M. Primary management of carcinoma of the breast. Lancet 1993;342:1402-8. 2. Ivens D, Hoe AL, Podd TJ, Hamilton CR, Taylor I, Royde GT. Assessment of morbidity from complete axillary dissection. Br J Cancer 1992;66:136-8. 3. Petrek JA. Axillary dissection: Current practice and technique. Curr Probl Surg 1995;32:267-323. 4. Kuehn T, Klauss W, Darsow M, Regele S, Flock F, Maiterth C, et al. Long-term morbidity following axillary dissection in breast cancer patients- clinical assessment, significance for life quality and the impact of demographic, oncologic and therapeutic factors: Breast Cancer Res Treat 2000;64:275-86. 5. McMasters KM, Giuliano AE, Ross MI, Reintgen DS, Hunt KK, Byrd DR, et al. Sentinel lymph-node biopsy for breast cancer - not yet the standard of care. N Engl J Med 1998;339;990-5. 6. Veronesi U, Paganelli G, Viale G, Galimberti V, Luini A, Zurrida S, et al. Sentinel lymph node biopsy and axillary dissection in breast cancer: results in a large series. J Natl Cancer Inst 1999;91:368-73. 7. Fisher B, Redmond C, Fisher ER, Bauer M, Wolmark N, Wickerham L, et al. Ten-year results of a randomised clinical trial comparing radical mastectomy and total mastectomy with or without radiation. N Engl J Med 1985;312:674-81. 8. Jatoi I. Management of axilla in primary breast cancer: Surg Clin North Am 1999;79:1061-73. 9. Stewart HJ, Everington D, Forest APM. The Cardiff local therapy trial results at 20 years. Breast 1994;3:40-5. 10. Stewart HJ, Jack WJL, Everington D, et al. South-east Scottish trial of local therapy in node negative breast cancer. Breast 1994;3: 31-9. 11. Forrest AP, Everington D, McDonald CC, Steele RJ, Chetty U, Stewart HJ. The Edinburgh randomized trial of axillary sampling or clearance after mastectomy: Br J Surg 1995;82:1504-8. 12. Steele RJ, Forrest APM, Gibson T, Stewart HJ, Chetty U. The efficacy of lower axillary sampling in obtaining lymph node status in breast cancer: a controlled randomized trial. Br J Surg 1985;72:368-9. 13. Ahlgren J, Liljegren G, Holmberg L, et al. Five-node biopsy of the axilla, an alternative to sentinel node biopsy in operable breast cancer (abstract no.274) Abstract book _ 2nd European Breast cancer conference. September 2000. Vol 36. pp. S98-S99. 14. Orr RK, Hoehn JL, Col NF. The learning curve for sentinel node biopsy in breast cancer: practical considerations. Arch Surg 1999;134:764-7. 15. Tafra L, Lannin DR, Swanson MS, Van Eyk JJ, Ve324rbanac KM, Chua AN, et al. Multicentre trial of sentinel node biopsy for breast cancer using both technetium sulphur colloid and isosulphan blue dye. Ann Surg 2001;233:51-9. 16. Cox CE, Pendas S, Cox JM, Joseph E, Shons AR, Yeatman T, et al. Guidelines for sentinel node biopsy and lymphatic mapping of patients with breast cancer. Ann Surg 1998;227:645-53. 17. Hill AD, Tran KN, Akhurst T, Yeung H, Yeh SD, Rosen PP, et al. Lessons learned from 500 cases of lymphatic mapping for breast cancer. Ann Surg 1999;229:528-35. 18. Giuliano AE, Dale PS, Turner RR, Morton DL, Evans SW, Krasne DL. Improved axillary staging of breast cancer with sentinel lymphadenectomy. Ann Surg 1995;222:394-401. 19. Paganelli G, De Cicco C, Cremonesi M, Prisco G, Calza P, Luini A, et al. Optimized sentinel node scintigraphy in breast cancer. Q J Nucl Med 1998;42:49-53. 20. Motomura K, Inaji H, Komoike Y, Kasugai T, Nagumo S, Noguchi S, et al. Sentinel Node Biopsy in Breast Cancer Patients with Clinically Negative lymph nodes. Breast Cancer 1999;6:259-62. 21. Motta C, Cartia G, Muni A, Giudici M, Falcetto G, Castaldo P, et al. Sentinel lymph node identification in breast cancer: feasibility study. Tumori 2000;86:304-6. 22. Cserni G, Rajtar M, Boross G. Blue nodes left behind after vital blue dye-guided axillary sentinel node biopsy in breast cancer patients. Jpn J Clin Oncol 2000;30:263-6 23. Cserni G, Boross G, Baltas B. Value of axillary sentinel nodal status in breast cancer. World J Surg 2000;24:341-4. 24. Winchester DJ, Sener SF, Winchester DP, Perlman RM, Goldschmidt RA, Motykie G, et al. Sentinel lymphadenectomy for breast cancer: experience with 180 consecutive patients: efficacy of filtered technetium 99m sulphur colloid with overnight migration time. J Am Coll Surg 1999;188:597-603. 25. Dunnwald LK, Mankoff DA, Byrd DR, Anderson BO, Moe RE, Yeung RS, et al. Technical aspects of sentinel node lymphoscintigraphy for breast cancer. J Nucl Med Technol 1999;27:106-11. 26. Ikeda T, Masamura S, Fujii H, Hiramatsu H, Mukai M, Matsui A, et al. Sentinel lymph node biopsy using Tin Colloid RI and Blue Dye method. Breast Cancer 2000;7:284-6. 27. Giuliano AE, Jones RC, Brennan M, Statman R. Sentinel lymphadenectomy in breast cancer. J Clin Oncol 1997;15:2345-50. 28. Chetty U, Jack W, Prescott RJ, Tyler C, Rodger A. Management of axilla in operable breast cancer treated by breast conservation: a randomized clinical trial. Br J Surg 2000:87;163-9. 29. Krag D, Weaver D, Ashikaga T, Moffat F, et al. The sentinel node in breast cancer: A Multicenter validation study. N Eng J Med 1998;339;941-6. 30. Dixon JM, Dillon P, Anderson TJ, Chetty U. Axillary node sampling in breast cancer: an assessment of its efficacy. Breast 1998;7:206-8. 31. Kutiyanawala MA, Sayed M, Stotter A, Windle R, Rew D. Staging the axilla in breast cancer: an audit of lymph-node retrieval in one U.K. regional centre. Eur J Surg Oncol 1998;24:280-2. 32. Badwe RA, Mittra I. Sentinel node biopsy in breast cancer. Lancet 2001;357:2054. 33. Macmillan RD, Barbera D, Hadjiminas DJ, Rampaul RS, Lee AH, Pinder SE, et al. Se ntinel node biopsy for breast cancer may have little to offer four-node samplers: results of a prospective comparison study. Eur J Cancer 2001;37:1076-80. 34. Wong SL, Edwards MJ, Chao C, Tuttle TM, Noyes RD, Carlson DJ, et al. Sentinel lymph node biopsy for breast cancer: Impact of the number of sentinel nodes removed on the false negative rate. J Am Coll Sorg 2001;192:684-91. 35. Clarke D, Khonji NI, Mansel RE. Sentinel node biopsy in breast cancer: ALMANAC trial. World J Surg 2001;25:819-22. 36. Grube BJ, Giuliano AE. Observation of breast cancer patient with a tumor positive sentinel node: Implication of the ACOSOG Z0011 trial. Semin Surg Oncol 2001;20:230-7. © 2003 Indian Journal of Surgery. Also available online at http://www.indianjsurg.com
The following images related to this document are available:Photo images[is03071t6.jpg] [is03071t2.jpg] [is03071t3b.jpg] [is03071t1.jpg] [is03071t5.jpg] [is03071t3c.jpg] [is03071t3a.jpg] [is03071t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}