 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 65, No. 4, July-Aug, 2003, pp. 366-367 Case Reports Breast metastsis of embryonal rhabdomyosarcoma of orbit Bhavana Rai, Sushmita Ghoshal, S. C. Sharma, R. Nijhawan,* Manishi Bansal Departments of Radiotherapy and *Pathology, Postgraduate Institute of Medical Education and Research, Chandigarh 160012.
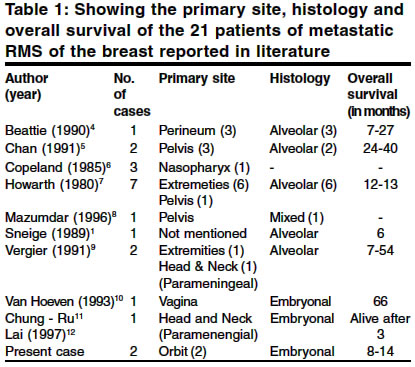
How to cite this article: Rai B, Ghoshal S, Sharma SC, Nijhawan R, Bansal M. Breast metastsis of embryonal rhabdomyosarcoma of orbit. Indian J Surg 2003;65:366-7. Paper Received: September 2002. Paper Accepted: January 2003. Source of Support: Nil Code Number: is03072 Abstract Metastatic malignancy of the breast is relatively uncommon. Extramammary tumours metastatic to the breast represent 5.1% of all breast cancers and commonly occur in adolescents and young adults. The propensity of tumours to metastasize to the breasts of young women has been attributed to the blood supply which increases during puberty and drops after menopause. Metastatic rhabdomyosarcoma is rare, with only 21 cases reported in the literature so far. We report 2 additional cases of embryonal rhabdomysarcoma with metastasis to the breast. Key Words: Rhabdomyosarcoma, Neoplasm, Metastasis, Embryonal, Breast neoplasm. Rhabdomyosarcoma (RMS), the most common malignant tumour of the soft tissue in infants and children has an incidence of 4.5 cases per million children. The most common primary site for RMS is the orbit. RMS are traditionally classified into pleomorphic, embryonal and alveolar orbit. The embryonal histology occurs in 60% cases and is found most commonly in the head and neck, orbit and genito-urinary sites. The most common sites of haematogenous dissemination are lungs, bone marrow, liver, and brain. Metastatic RMS of the breast is rare. The subtype most commonly associated with metastatic RMS of the breast is alveolar type, the primary site being the extremities. However, in our cases the RMS was embryonal and the primary site was orbit. RMS with this histological subtype and occuring at this site carry a relatively better prognosis. Therefore, we report 2 cases of metastatic RMS of the breast. Case Reports Case 1 A 16-year-old female was diagnosed in May 1999 with embryonal RMS of the orbit. The patient had multiple bilateral cervical nodes. The patient received 3 cycles of chemotherapy with vincristine, adriamycin and cyclophosphamide followed by radiation therapy 55 Gy/25 fractions/5 weeks, to the orbit. The patient had a partial response to treatment. A single, non-tender swelling in the left breast about 4x4 cm in size, in the left upper outer quadrant was noticed in January 2000. Needle aspiration cytology done to evaluate the breast mass was reported to be consistent with embryonal RMS. The patient was started on second line chemotherapy with ifosfamide, cisplatin and etoposide. However, the disease progressed and the patient expired in August 2000. Case 2 A 22-year-old married female was diagnosed in June 2000 with embryonal RMS of the left orbit. Though the disease was locally advanced, there was no evidence of distant metastasis. The patient received treatment with chemotherapy, 3 cycles with vincristine adriamycin, cyclophosphamide followed by radiation therapy 40 Gy/ 20 fractions/4 weeks, to the orbit. A complete response was shown after completion of treatment. After 12 months of follow-up, a 6x6 cm swelling was a noticed occupying 3/4th of the breast. Fine needle aspiration was done to evaluate the mass and which reported as embryonal RMS. The patient received treatment with radiation therapy to the left breast and draining axilla. A dose of 40Gy in 20 fractions over 4 weeks was delivered by 2 lateral tangentials and an incident dose of 45 Gy in 20 fractions was delivered for 4 weeks to the axillary and supraclavicular area. Two months later, the patient was found to have a local recurrence in the orbit. The patient refused further treatment and did not come for follow-up thereafter. DISCUSSION Metastasis to the breast from extramammary tumours is relatively uncommon and represents only 5.1% of breast cancers. The common extramammary tumours that metastasize to the breast are malignant melanoma, lymphoma, bronchogenic carcinoma, followed by a smaller number of primary tumours from the GI tract, genitourinary tract and rarely, RMS.1 Metastasis to the breast in the young is attributed to the increase in the blood supply to the developing breast.2 Pettinatto et al3 reviewed 113 tumours of the breast in adolescents and found 8 metastatic malignant tumours, out of which 3 were habdomyosarcomas of the alveolar type. A review of the literature revealed only 21 cases of metastatic RMS of the breast (Table 1). Only 4 out of the 21 cases were of the embryonal subtype. The age group ranged from 11- 30 years and the median age at diagnosis was 15 years. 19 out of 21 patients were females and the primary site in most cases was the extremities and perineum. 1 case each was of the maxillary sinus and nasopharynx. Most of the cases had advanced disease at the time of presentation of metastasis and the interval between the primary and the breast metastasis ranged from 0 to 48 months. Our cases differed from the previous reported ones in that both the patients had the primary sites as orbit which carries a relatively good prognosis as compared to the alveolar subtype. The age of the patients was 16 and 22 years. The overall survival was 9 months and 8 months respectively. To conclude, breast metastases from embryonal rhabdomyosarcoma with the primary site as orbit is extremely rare. Metastasis to the breast is more common in young females, perhaps due to an increase in the vascularity of breast tissue and carries a poor prognosis. REFERENCES 1. Sneige N. Zachariah S, Janning TV, Dekmezian RH, Ordonez NG. Fineneedle aspiration cytology of metastatic neoplasms of breast. Am Clin Pathol 1989;92:27-35. 2. Deeley TJ. Secondary depostis in the breast. Br J Cancer 1965;19:738-43. 3. Pettinato G, Manivel JC, Kelly DR, Wold LE, Dehner LP.Lesions of the breast in children exclusive of typical fibroadenoma and gynecomastia. A clinicopathologic study of 113 cases. Pathol Annu 1989;24:296-328. 4. Beattie M, Kingstor JE, Nortan AJ, Malaps JS. Nasopharyngeal rhabdomyosarcoma presenting as a breast mass. Pediatr Hematol Oncol 1990;7:25:9-263. 5. Chan KW, Rogers PCJ, Tryer CJH. Breast metastasis after bone marrow transplantation for rhabdomyosarcoma. Bone Marrow Transplant 1991;7:171-2. 6. Copeland LJ, Soneige N, Stinger AS, Gerhenson DM, Saul PB, Kavanagh JJ. Alveolar rhabdomyosarcoma of the female genitalia. Cancer 1985;849-55. 7. Howarth CB, Caces JN, Praff CB. Breast metastasis in children with rhabdomyosarcoma. Cancer 980;46:2520-4. 8. Mazumdar GA, Murthy AK. Bilateral mammory metastasis of alveolar soft part sarcoma - A case report. Indian J Pathol Microbiol 1996;39:325-7. 9. Vargier B, Trajani M, Mascarel ID, Coindre JM, Treut AL. Metastasis of the breast. Differential diagnosis from primary breast carcinoma. J Surg Oncol 1991;48:112-6. 10. Von Hoeven KH, Hubbord CA, Flax H, Jones JG, Subrland MJ. Metastatic malignant neoplasms and secondary lymnphomatous involvement of the breast. A study of 43 cases. Pathol Ann 1993;28:221-41. 11. Chung RL, Chih YH, Shyh HT, Hung C. Adult embryonol Rhabdomyosarcoma metastatic to the breast and diagnosed by fine needle aspiration. Acta Cytologica 1997; 41:845-8. 12. Asmar L, Gehan EM, Newton WA, Webber BL, Marsden HB, van Unnik AJ, et al. Agreement among and within groups of pathologists in the classification of rhabdomyosarcoma and related childhood sarcomas: Report of an international study of four pathology classifications. Cancer 1994;74:2579-88. © 2003 Indian Journal of Surgery. Also available online at http://www.indianjsurg.com
The following images related to this document are available:Photo images[is03072t1.jpg] |
| |||||||||

{kind=link}