 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 65, No. 4, July-Aug, 2003, pp. 370-371 Case Report |
Anorectal amelanotic malignant melanoma Prosanta Kumar Bhattacharjee, Debabrata Ray, Manimala Ray,* Jayati Mitra,* Sagar Sadhu Departments of Surgery and *Pathology, R G Kar Medical College, Kolkata 700 004, West Bengal.
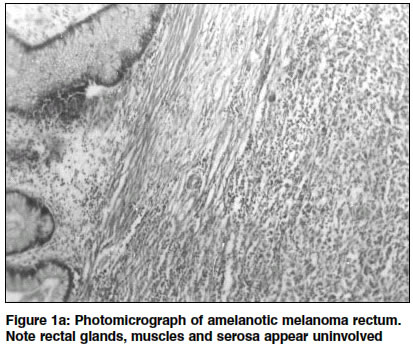
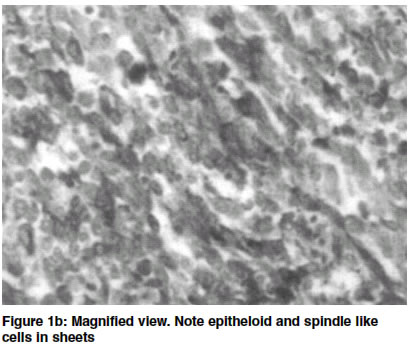
How to cite this article: Bhattacharjee PK, Ray D, Ray M, Mitra J, Sadhu S. Anorectal amelanotic malignant melanoma. Indian J Surg 2003;65:370-2. Paper Received: July 2002. Paper Accepted: August 2002. Source of Support: Nil Code Number: is03074 Abstract A 45-year-old lady presented with history of painless bleeding per rectum for 2 months. Colonoscopy revealed a small growth involving the region of the anorectal junction, biopsy of which was reported to be poorly differentiated carcinoma, with the possibility of amelanotic melanoma. At the time of undergoing abdominoperineal resection the patient did not show any obvious evidence of regional lymph node involvement or distant metastases. Histopathology of the tumour after routine haematoxylin and eosin (H&E) stain and subsequent special staining with anti-melanoma antibodies, HMB 45 and S 100, conclusively proved amelanotic melanoma. She developed multiple secondary deposits in the liver after 3 months of surgery and a recent bone scan revealed multiple metastases in the bones. However, she is still alive at the time of reporting. Key words: Amelanotic Melanoma, Rectum, Anal canal. Introduction Malignant melanoma of the anorectum is a rare tumour and the amelanotic variety is even more uncommon.1 These tumours mainly arise from the transitional zone of the surgical anal canal from the melanocytes normally present at that site.2 Not infrequently are they amelanotic.3 Extracutaneous amelanotic melanoma can present diagnostic problems in histopathology. Macroscopically, the tumours lack pigmentation and microscopically they are deficient in melanin, however they show positive staining with HMB-45 and S 100 protein, the anti-melanoma antibodies. We report a rare case of amelanotic melanoma of the anorectum in a middle-aged lady. Case report A-45-year-old lady presented with history of painless bleeding per rectum after every motion for 2 months and generalized weakness and weight loss for 1 month. On examination, the patient looked frail, pale and weighed 47 kg. Cervical and inguinal lymph nodes were not enlarged. Per abdominal examination did not reveal any abnormalities. Per rectal digital examination revealed a hard, sessile, non-tender mass 4 to 5 cm from the anal verge, which bled on touch. No other abnormality was noticeable on clinical examination. Hematological examination revealed the hemoglobin to be 7.2 gm%, but the biochemical parameters including liver function as well as carcinoembryonic antigen (CEA) were normal. A plain x-ray of the chest and ultrasonography (USG) of the abdomen did not reveal any abnormality. Colonoscopy showed a posteriorly located, non-pigmented, sessile mass approximately 1.5 cm in diameter with central ulcer, extending from the anorectal junction to the lower part of the rectum. Rest of the colon was normal. Histopathology report of the colonoscopic biopsy specimen showed a poorly differentiated carcinoma with the possibility of amelanotic melanoma. The patient underwent an abdominoperineal resection after correction of anaemia . At the time of surgery she did not show any obvious evidence of either regional or distant spread of the tumour. The excised specimen on being cut open showed a sessile, non-pigmented growth, 1.8 cm x 1.5 cm, arising from the posterior aspect of the anorectum, 5 cm from the anal verge. The growth had a central ulcer and the surrounding mucosa was normal. Microscopic examination of sections from the upper part of the growth showed epitheloid and spindle like cells in sheets. Rectal glands, muscle coats and serosa were uninvolved (Figures 1a & b). Sections from the lower part of the growth also showed similar sheets of cells. Since the histological picture suggested the possibility of amelanotic melanoma, immunohistochemical staining with HMB 45 and S100 protein was performed. Positive staining confirmed the lesion to be amelanotic melanoma. The cut margins of the specimen and the lymph nodes removed along with it did not show any tumour deposit. Routine USG screening of abdomen during follow-up showed multiple secondary deposits in the liver 3 months after surgery and a bone scan done later for back pain revealed metastases in the bones. Discussion Although malignant melanomas arise most commonly from the skin, they may rarely arise from the melanocytes present at extracutaneous sites as well. Malignant melanoma of the anorectal region is rare and comprises approximately 1-3 % of the anal canal cancers,1,2 around 30% of which are amelanotic.3 Arising close to the pectinate line it grows towards the rectal ampulla, as in this reported case, sometimes emerging through the mucous membrane at a higher point, simulating primary rectal carcinoma. Preoperative diagnosis of amelanotic melanoma, especially at extracutaneous sites, is difficult. Microscopically they lack melanin pigment but on immunohistochemical staining the typical melanomas show positive staining with HMB 45 and S 100 protein (melanoma-specific antibodies). HMB 45 is a more specific marker than S 100 protein as the latter may react positively to some non-melanocytic tumours like breast carcinoma. The commonest presenting symptom is bleeding, as in our case, others are pain, mass, ulcer, diarrhoea and tenesmus.4 They may often be misdiagnosed as thrombosed piles, diagnosis in such cases is made on histological examination of the excised haemorrhoids. Anorectal melanomas have a very poor prognosis, around 60% have clinically evident regional or distant metastases at the time of diagnosis. Even though not clinically evident, as was true in our case, most of them are disseminated at the time of presentation.4 Ideal treatment of anorectal melanomas still remains controversial, with 90% of the patients dying irrespective of the surgical approach or multidisciplinary treatment.5 Recommended surgical procedures vary from posterior pelvic exenteration at one extreme, less radical abdominoperineal resection (APR) with or without inguinal lymph node dissection to conservative wide local excision (WLE) again with or without inguinal lymph node dissection. Some, like Cooper et al,2 advocate APR because of more effective local control and since it removes clinically undetectable lymph nodes. While others like Ward et al4 suggested WLE with a 2-cm margin along with therapeutic inguinal lymph node dissection for positive nodes, as majority of the patients have metastases at the time of diagnosis and survival is not significantly better with radical surgery. Moreover, WLE effectively controls local symptoms while maintaining continence. However, though chances of local recurrence are minimized there was an instance where APR had to be resorted to after WLE because of rectal obstruction from pelvic nodal recurrence.4 Our patient who had presented early with a small growth came from a poor family. We had opted for APR to obviate any future major exploration either due to local or pelvic nodal recurrence. Moreover, the patient herself had wished a radical surgery knowing fully well that she would have to live with a colostomy. References 1. Gobel D, Vorphal U, Schafer A, Henneking K, Terpe HJ. Amelanotic melanoma of the rectum. Chirurg 1993;64:829-31. 2. Cooper PH, Mills SE, Allen MS Jr. Malignant melanoma of the anus: report of 12 patients and analysis of 255 additional cases. Dis Colon Rectum 1982;25:693-703. 3. Nozoe T, Anai H. Amelanotic malignant melanoma of the rectum: report of a case. Surg Today 2001;31:527-9. 4. Ward MWN, Romano G, Nicholls RJ. The surgical treatment of anorectal malignant melanoma. Br J Surg 1986;73:68-9. 5. Shank B, Enker WE Neoplasm of the anus. In: Holland JF, Bast RC Jr, Morton DL, Frei E III, Kufe DW, Weichselbaum RR, editors. Cancer Medicine. 4th edn. Baltimore: William and Wilkins; 1997. Vol 2. pp. 2073-82. © 2003 Indian Journal of Surgery. Also available online at http://www.indianjsurg.com
The following images related to this document are available:Photo images[is03074f1b.jpg] [is03074f1a.jpg] |
| |||||||||

{kind=link}
{kind=link}