Cutaneous metastases from gastric carcinoma
Shivananda Prabhu, K. Ramchandra Pai, Erel A. I. Diaz, Shubha Rao, Vamsi Krishna
Department of Surgery, Kasturba Medical College Hospital, Attavar, Mangalore 575001.
Address for correspondence Dr. Shivananda Prabhu, Department of Surgery, Kasturba Medical College Hospital, Attavar, Mangalore 575001, Karnataka.
How to cite this article: Prabhu S, Pai KR, Diaz EAI, Rao S, Krishna
V. Cutaneous metastases from gastric carcinoma. Indian J Surg 2003;65:372-3.
Paper Received: June 2002. Paper Accepted: August 2002. Source of Support: Nil
Code Number: is03075
Abstract
Cutaneous metastases are uncommon. Breast, lungs and abdominal viscera are the common sites of
primary tumour in patients presenting with cutaneous metastases. Prognosis for such patients is poor though
chemotherapy may offer some benefit. The role of surgery is palliative. We report a 25-year-old man with adenocarcinoma of
the stomach who developed tumour deposit in the skin of the face.
Key words:
Metastasis, Cancer stomach, Skin, Cutaneous.
Introduction
Internal malignancies rarely metastasize to
the skin.1,2 Head and neck and trunk are the
common sites for skin deposits.1,3 We report a
25-year-old man with adenocarcinoma of the stomach
who developed tumour deposit in the skin of the face.
Case report
A 25-year-old man presented with history
suggestive of gastric outlet obstruction for 3 months.
Endoscopy showed an ulceroproliferative growth in the
gastric antrum, biopsy from which showed
adenocarcinoma. At laparotomy, as the growth was unresectable a palliative gastrojejunostomy was done. The patient
was advised palliative chemotherapy following
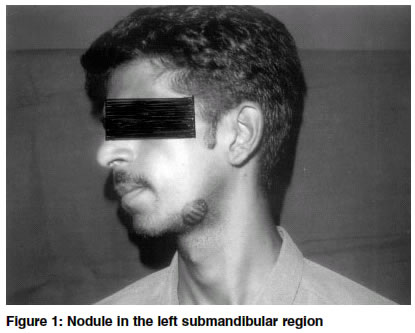
surgery. During the course of chemotherapy a small nodule
was noticed in the left mandibular region (Figure
1). Aspiration cytology from the nodule confirmed
the suspicion of metastasis from gastric carcinoma.
After the third cycle of chemotherapy the patient was lost
to follow-up.
Discussion
The skin is rarely involved in
metastases.1,3 When cutaneous deposits do occur, the primary is
usually found in the breast, lungs or abdominal
viscera.2 Head and neck, chest and the abdominal wall are
the commoner sites of cutaneous metastatic
deposits.1
Rarely, such metastases may be the first sign of the
disease.3 The diagnosis is by fine needle aspiration from
the skin nodule. When the primary is not known
histopathology of the skin metastasis might offer a clue
to its site.3
A study by Hori et al showed that the average interval between the detection of the primary cancer and
the appearance of the skin lesion was 20
months.4 Prognosis is usually poor owing to the presence
of widespread metastases. Chemotherapy has been reported to improve survival in some
patients.5 The role of surgery is limited to palliating the
complications of the primary.
References
1. Boscanio A, Orabona P,
D'Antonio, Staibano S, De Rosa G. Cutaneous metastases from gastric adenocarcinoma. Report of
two cases and review literature. Arch Anat Cytol Pathol 1996;44:
60-4.
2. Miwa M, Matsumura H, Miwa T, Sato S. A young gastric
carcinoma patient with umbilical and scrotal metastasis. Tokai J
Exp Clin Med 1981;6:305-8.
3. Descamps V, Makhlouf R, Katchourine I, Grossin M, Belaich
S. Linitis plastica disclosed by cervical cutaneous metastasis.
Ann Dermatol Venereal 1995;122:108-10.
4. Hori M, Yoshida H. Statistical study of metastatic skin cancers
interrelation of the origin of primary tumor,metastatic skin
lesions, prognosis and histopathology. Gan To Kagaku
Ryoho 1988;15:1576-80.
5. Tajima H, Matsuki N, Takeda T, Horichi H, Kumaki T, Shima K.
A case of cutaneous and brain metastasis of gastric carcinoma
treated effectively by chemotherapy with CDDP, MMC, etoposide
and 5'-DFUR. Gan To Kagaku Ryoho 1994;21:2659-62.
© 2003 Indian Journal of Surgery. Also available online at http://www.indianjsurg.com


{kind=link}