 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 65, No. 4, July-Aug, 2003, pp. 373-374 Case Report Bilataeral adrenal metastases from bilateral small cell neuroendocrine carcinoma of the ovary Shirley Sundersingh, Sundaram Rajasundaram, Urmila Majhi Department of Pathology, Cancer Institute (WIA), 18, Sardara Patel Road, Chennai 600036.
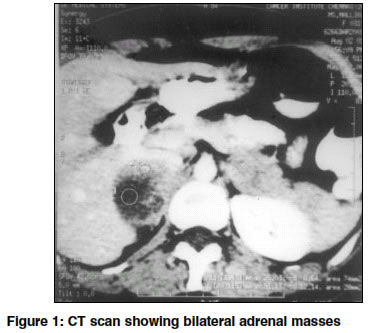
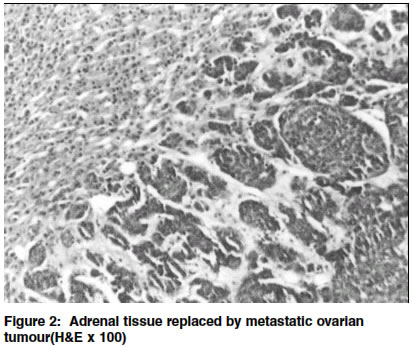
How to cite this article: Sundersingh S, Rajasundaram S, Majhi U. Biltaeral adrenal metastases from bilateral small cell neuroendocrine carcinoma of the ovary. Indian J Surg 2003;65:373-5. Paper Received: June 2002. Paper Accepted: August 2002. Source of Support: Nil Code Number: is03076 Abstract A 31-year-old female was referred to our institute following total abdominal hysterectomy with bilateral salpingo-oophorectomy done elsewhere for a pelvic mass diagnosed as bilateral ovarian tumour. Further investigations revealed bilateral adrenal masses for which she underwent bilateral adrenalectomy. Histological examination of both the ovarian and adrenal tumours revealed features of small cell neuroendocrine carcinoma of the ovary. These are rare ovarian tumours and metastases from them to the adrenal glands has not been reported so far. Key words: Ovary tumour, Adrenal metastases, Small cell neuroendocrine carcinoma. Introduction Adrenal glands are rare sites of distant metastases, the common primary being breast, lungs, stomach and colon. Metastases from the ovary are very rare.1 Adrenal metastases were usually found at autopsy, however, now with improved imaging techniques, increasing numbers of these are being detected before death. A rare case of bilateral adrenal metastases from bilateral ovarian small cell neuroendocrine carcinoma is discussed here. Small cell neuroendocrine carcinomas of the ovary are a rare heterogenous group of neoplasms with endocrine differentiation potential. They are thought to be of surface epithelial origin.2 Metastases of these tumours to the adrenal glands have not been reported so far. Case report A 31-year-old lady was referred to our institute with a past history of abdominal distension and lower abdominal pain of 2 months duration. She was diagnosed as having bilateral ovarian masses and had undergone total abdominal hysterectomy with bilateral salpingo-oophorectomy elsewhere. The postoperative histopathology was reported as bilateral poorly differentiated carcinoma of the ovary, Grade III. She had also received 1 cycle of chemotherapy. Examination at our centre revealed the patient to be in good health with a well-healed midline scar. Review of the prior histopathology slides showed features of an undifferentiated carcinoma of the ovary, Grade III, probably of neuroendocrine origin. CT scan of the abdomen revealed bilateral, complex suprarenal masses with hypoechoic centre and irregular capsule measuring 5x2.7x2.8 cm on the right side and 3.5x3.3x2.6 cm on the left side (Figure 1). The centre was non-enhancing, while the periphery showed good contrast enhancement. There was no calcification or infiltration of the adjacent organs. Urinary VMA, serum cortisol, serum DHEAS, urinary 17-ketosteroids and cortisol levels were within normal limits. There were no signs of virilization, adrenal insufficiency or hypertension. Other serum markers like CA-125 and CEA were within normal limits. Upper gastrointestinal endoscopy, CT chest and bone scan were normal. Fine needle aspiration of the adrenal mass was done but was inconclusive. Since the patient was in good general condition and there was no evidence of metastases elsewhere in the body, excision of the bilateral adrenal masses was done. The postoperative period was uneventful. On gross examination, the excised specimens both had a well-defined, smooth surface, with the cut sections revealing areas of haemorrhage. Microscopic examination revealed adrenal tissue replaced by a tumour with morphology similar to an ovarian tumour (Figure 2), composed of cells arranged in small clusters, nests, alveolar masses, sheets, in a trabecular and glandular pattern. The cells were small to medium-sized with scanty cytoplasm and hyperchromatic nuclei with inconspicuous nucleoli separated by scanty to moderate fibrous stroma. Mitotic activity was increased. Immunohistochemistry of both the ovarian and adrenal tumours showed a strong positivity of the tumour cells for Chromogranin A, Synaptophysin, Neuron-specific enolase, Epithelial membrane antigen and Keratin. Stain for Vimentin was negative. Taking histology and immunology into consideration a diagnosis of bilateral small cell neuroendocrine carcinoma of the ovary with bilateral adrenal metastases was made. Discussion Small cell neuroendocrine carcinoma of the ovary is a rare entity. The most common differential diagnosis for this tumour is adult granulosa cell tumour. The former is differentiated from the latter based on its neuroendocrine differentiation (which was confirmed by immunohistochemistry in our case). Adrenal metastases used to be a postmortem finding in the past. With the advent of improved imaging modalities these are detected at an earlier stage. CT scan particularly, has been shown to be both specific and sensitive in detecting them3 and hence an increasing number of adrenal metastases are now being identified. The management of patients with adrenal metastases poses a therapeutic challenge. Although they were once considered incurable, surgery has been recommended for isolated metastasis. Adrenalectomy for metastatic cancer was rarely performed since the survival benefit for patients undergoing such resections was not clear. However, it has been advised in cases where there is unilateral adrenal metastasis with no residual primary or other distant metastasis with good performance status of the patient.4 Patients with long disease-free intervals and favourable tumour biology should also be offered resection since such patients have a long-term survival. Bilateral metastases have rarely been encountered and surgical treatment is seldom performed in these cases, since it is thought that other metastatic foci are usually concomitant. However, several cases have been reported with prolonged survival of the patient following bilateral adrenalectomy for tumours of the lung, colon, breast and kidney. Adrenal metastases are often large at the time of diagnosis. Since surgical resection is a safe procedure and more patients could be alive for a long time, it should be performed whenever possible.5 Moreover, surgical resection for metastases to the adrenal glands is associated with low mortality and morbidity rates. Our patient is alive and healthy with no evidence of any other metastases one year after surgery. REFERENCES 1. Cedermark BJ, Blumenson LE, Pickren JW, Holyoke DE, Elias EG. The significance of metastases to the adrenal glands in adenocarcinoma of the colon and rectum. Surg Gynecol Obstet 1977;144:537-46. 2. Eichhorn JH, Young RH, Scully RE. Primary ovarian small cell carcinoma of pulmonary type: a clinicopathologic, immunohistochemical and flow cytometric analysis of 11 cases. Am J Surg Path 1992;16:926-38. 3. Pagani JJ. Non-small cell lung carcinoma adrenal metastases: computed tomography and percutaneous needle biopsy in their diagnosis. Cancer 1984;53:1058-60. 4. Folli S, Zaccaroni A, Mengozzi M, Dell' Amore D, Vio A. Surgical treatment of adrenal metastases. Personal experience. Minerva Chir 1998;53:1035-8. 5. Shuto T, Hirohashi K, Kubo S, Tanaka H, Yamamoto T, Higaki I, et al. Treatment of adrenal metastases after hepatic resection of a hepatocellular carcinoma. Dig Surg 2001;18:294-7. © 2003 Indian Journal of Surgery. Also available online at http://www.indianjsurg.com
The following images related to this document are available:Photo images[is03076f1.jpg] [is03076f2.jpg] |
| |||||||||

{kind=link}
{kind=link}