 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
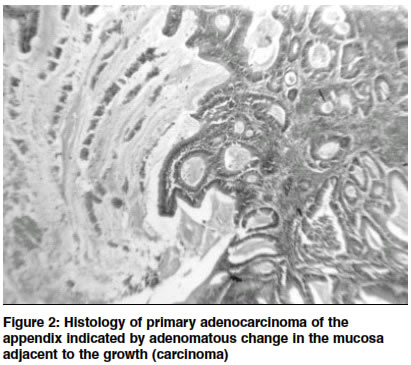
Indian Journal of Surgery, Vol. 65, No. 4, July-Aug, 2003, pp. 375-376 Case Report Primary adenocarcinoma of the appendix Leo Francis Tauro, Clement R. S. D'Souza, Hilda Fernandes,* H. W. Furtado, Leo Theobald Menezes Department of General Surgery and *Pathology, Fr. Muller's Medical College & Hospital, Kankanady, Mangalore 575002, Karnataka.
How to cite this article: Tauro LF, D'Souza CR, Fernandes H, Furtado HW, Menezes LT. Primary adenocarcinoma of the appendix. Indian J Surg 2003;65:375-7. Paper Received: January 2001. Paper Accepted: October 2001. Source of Support: Nil Code Number: is03077 Abstract Primary adenocarcinoma of the appendix is a rare neoplasm; less than 200 cases have been reported. We report a patient who underwent appendicectomy for acute appendicitis and on histopathological examination was found to have primary adenocarcinoma of the appendix. She underwent right hemicolectomy as a second stage operation. Key words: Adenocarcinoma, Appendix. Introduction Primary adenocarcinoma of the appendix is a rare neoplasm comprising less than 0.5% of all gastrointestinal neoplasms.1,2 We report a patient in whom the appendicectomy specimen revealed a neoplasm of the appendix. Case report A 63-year-old woman presented with a history of abdominal pain, vomiting and fever for 2 days. She was febrile. Abdominal examination revealed rebound tenderness in the right iliac fossa. Rectal examination was normal. Haematological investigations revealed a raised leucocyte count with neutrophilia. Urine and other blood investigations were normal. Ultrasonography of the abdomen showed inflammed, thickened appendix. She undwerwent open appendicectomy. At surgery the appendix was found to be turgid and thickened. On gross sectioning, a greyish white growth with tiny areas of necrosis was found to occupy the lumen of the appendix with a cystic area filled with mucinous material distally (Figure 1). Histological examination diagnosed a well-differentiated primary adenocarcinoma of the appendix (mucinous type) with Duke's grade A, (Figure 2) The tumour clearance was considered to be incomplete. Ten days later she underwent right hemicolectomy through right paramedian incision. At surgery, no palpable growth was identified in the caecum, nor any secondary deposits. Histopathological examination of the specimen showed only residual tumour at the appendicular stump but no malignancy in resected caecum, colon and regional lymph nodes. She made an uneventful recovery, and subsequently received 6 cycles of chemotherapy with endoxan and 5-fluorouracil at monthly intervals. A year later she remains asymptomatic with no evidence of any recurrence or metastases. Discussion Primary adenocarcinoma of the appendix is common during or after the 5th decade of life though an occasional paediatric case report is seen.3 Only 200 cases have been reported so far. The incidence of primary adenocarcinoma of the appendix is between 0.01 to 0.11 of all appendicectomies. The first case was reported by Berger in 1882. Gilhome and associates reported a series of 10 cases of adenocarcinoma appendix. Clinically, most of them present as acute appendicitis or appendicular mass.4 Hence it has been suggested that in patients over the age of 50, appendicectomy should be done by laparotomy. Occasional cases may present with malaena or absence of leukocytosis or perforation. Cases presenting as ovarian cystadenocarcinoma may be seen.5 Histologically, adenocarcinoma of the appendix may have colonic or mucinous glands; rarely, cystadenocarcinoma or pseudomyxoma peritonei occurs.5 However, the findings of adenomatous change in the mucosa adjacent to the growth (carcinoma) is the best evidence that the latter is primary. Appendicectomy alone is sufficient if the tumour is in the distal part of the viscus and confined to the submucosa, otherwise right hemicolectomy is indicated.4 Prognosis is better in the mucinous type than in the colonic type. Pseudomyxoma peritonei has bad prognosis. Overall prognosis was best understood in a review of 94 cases from 1976-1992. Five-year survival rate was 55%. It varied with stages and grades. Stage A 100%, Stage B 67%, Stage C 52%, Stage D 6% and low-grade 68%, high-grade 7%. References 1. Lee SS, Song KT. Primary adenocarcinoma of the appendix: a case report of two cases. J Surg Oncol 1982;21:162-4. 2. Nitecki SS, Wolff BG, Schlinkert R, Sarr MG. The natural history of surgically treated primary adenocarcinoma of the appendix. Ann Surg 1994;219:51-7. 3. Driver CP, Bowen J, Bruce J. Adenocarinoma of the appendix in a child. J Paed Surg 1998;33:1437-8. 4. Michael J, Zinner, Seymour I, Shwartz, Harold Ellis. Appendix and appendicectomy - Maingot's abdominal operations, 10th edn. Vol II. pp. 1191-228. 5. Skaane P, Sauer T, Jarve F. Mucinous adenocarcinoma of the appendix presenting as an ovarian cyst-adenocarcinoma: case report and review of appendiceal neoplasms with ovarian metastasis. Eur J Surg Oncol 1986;12:379-84. © 2003 Indian Journal of Surgery. Also available online at http://www.indianjsurg.com
The following images related to this document are available:Photo images[is03077f2.jpg] [is03077f1.jpg] |
| |||||||||

{kind=link}
{kind=link}