 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 65, No. 5, Sept-Oct, 2003, pp. 405-412 Review Article Indwelling JJ ureteral stents-A current perspective and review of literature Iqbal Singh Department of Surgery, University College of Medical Sciences (University
of Delhi) & GTB Hospital, Delhi, India.
Paper Received: November 2002. Paper Accepted: January 2003. Source of Support: Nil. How to cite this article: Singh I. Indwelling JJ ureteral stents-A current perspective and review of literature. Indian J Surg 2003;65:405-12. Code Number: is03080 ABSTRACT Aims & Introduction: To provide the surgeon with
information and physical data so as to optimize the safety and efficiency of
the ureteral stents in their patients. To review the current literature on
the use, implications and complications of indwelling double-J (DJ) ureteral
stents. To review the properties and qualities of various types of available
stents and the biomaterials used to manufacture them.
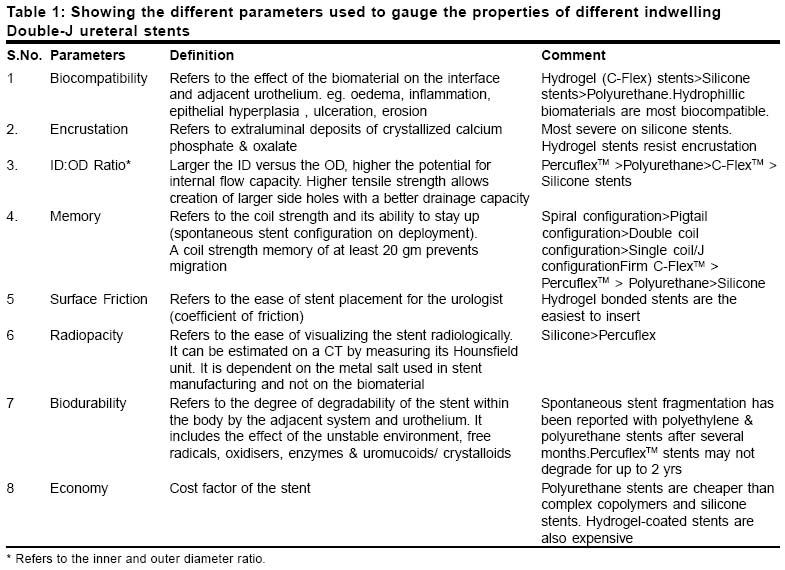
KEY WORDS: Stent complications, Encrusted stents, Polyurethane stents, Hydrophilic stents, Forgotten stents, DJ stents, Indwelling ureteral stents. INTRODUCTION There are numerous types of stents available in the market today. It is essential that those using them be familiar with their properties, design and demerits. There are no universal guidelines regarding their use, handling and effect. Despite tremendous advances in stent biomaterials and design, JJ stents are not free of complications and problems and the search for an ideal JJ stent may remain utopian.1,2 A literature search of various ureteral stents was carried out and depicted so as to have a broad overall view of ureteral stents and their recent advances. THE IDEAL STENT An ideal stent is expected to stay up and drain well. It should keep the biological passage open. It is expected to be patient-friendly and comfortable, free of complications even with prolonged indwelling times. It should also be biocompatible, biodurable and radioopaque. With such high expectations, tremendous improvements have taken place in the field of stent biomaterials, design and texture, however, the ideal stent continues to elude us.1,2 Thus the goal of ureteral stenting is to have a stent that will slide up, stay there, drain well, be comfortable to the patient, be easily visible on fluoroscopy and provide cost benefit to the patient and hospital. Table 1 shows the stent parameters that have been used to evaluate the properties of different stents. MATERIAL AND METHODS Various stent biomaterials that have been commonly used till date the world over have been depicted in Table 2 along with their composition and average tensile strength.3 JJ stents are prone to encrustation, a major problem that may limit its long-term use. Experimental studies have shown that various biomaterials may vary in their tendency towards encrustation. According to one such study,4 silicone was found to be the least prone to struvite encrustation, followed by polyurethane, silitek, percuflex and hydrogel-coated polyurethane.3 Similarly, silicone was also least susceptible to hydroxyapatite encrustation, followed by silitek, polyurethane, percuflex and hydrogel-coated polyurethane stents.4 According to Cormio et al, hydrogel-coated polyurethane stents such as Hydro-PlusTM cause minimal superficial epithelial destruction, show least ureteric reactive changes and low encrustation rates.5 It is believed that PercuflexTM stents (thermoplastic copolymer of polyolefin) have a high tensile strength with the best internal:outside diameter (ID:OD) ratios and an excellent side hole characteristic. A larger ID/OD ratio predicts an overall improved flow capacity of the stent. Moreover, the PercuflexTM stent has good biodurability and biocompatibility with good surface features and a low friction coefficient even without a hydrogel coating.4 According to Mardis et al3 polyurethane stents have questionable bio-durability and biocompatibility, hence these are suitable only for short-term deployment. INDICATIONS FOR URETERAL STENTING Broadly speaking the indications for ureteral stenting may be divided into two main headings, (a) As adjunct to Ureteral surgery (pre and/or postoperative), and (b) For managing ureteral obstruction (extrinsic and/or intrinsic). The salient indications6-14 for ureteral stenting are: (i) Adjuct to ESWL, PCNL, ureteroscopy, endopyelotomy, open/laparoscopic ureteral surgery, ureteric injury and renal transplantation. (ii) Managing ureteral obstruction (stones, strictures, oedema, fistula, tumours, tuberculosis, retroperitoneal fibrosis-tumours, hydronephrosis) and conservative management of genitourinary fistulas in women.14 Pre-ESWL stenting for renal stones (1-2 cm) and less than 1 cm ureteric stones is most controversial at the moment.12 It is important that the stenting should be done in selected cases only, even when indications do exist and not on a routine basis. According to Mardis et al2 approximately 50% of all extracorporeal lithotripsy and over 90% of all ureteroscopic stone procedures involve an indwelling ureteral stent. Thus the DJ stent is vital to the endourologist. Barely 10% of stenting is related to long-term stenting.24 Percutaneous nephrostomy drainage should be preferred where long-term stenting is anticipated such as in extrinsic obstruction by advanced abdominal malignancies.13 STENT COMPLICATIONS The common problems and complications encountered with indwelling ureteral DJ stents are enumerated below. Some of these complications are often related to prolonged indwelling times, especially in forgotten or overlooked stents.15-27 Early complications (i) Bladder storage symptoms and stent colic
Late complications (i) Hydronephrosis
STENT PAIN Stent pain refers to a constellation of clinical symptoms associated with the presence of a stent in the urinary tract. One must remember that JJ stents are foreign bodies that are prone to cause irritation and patient discomfort. Although silicone stents were more patient-friendly as these were seen to be better tolerated by patients, they are now almost phased out since they were less rigid, making their handling and insertion a tedious task.17 All JJ stents tend to cause discomfort on account of several factors such as stent rigidity/stiffness, stasis, long intravesical segments, migration and sepsis.18 This may lead to stent colic and pain with an impaired health-related quality of life.19,20 Soft stents produce significantly less severe stent discomfort than the firm stents. Stent Encrustation Polyurethane stents are especially prone to encrustation; this may be due to their higher tensile strength that contributes to their rigidity that may encourage stasis with periluminal and endoluminal encrustation. Biochemical and optical analyses of stent encrustations by Robert et al21 revealed that these encrustations consist mainly of calcium oxalate, calcium phosphate and ammonium magnesium phosphate. According to one study the stent encrustation rate increased from 9.2% at <6 wks, through 47.5% at 6-12 wks to 76.3% at >12 weeks.21 Up to a 30% rate of luminal blockage has been documented with indwelling times of up to 3 months and another 4% develop evidence of clinical obstruction.22 This occurs because a significant peri-stent drainage continues to occur, rather than urinary flow via the hollow stents. These problems tend to occur especially in those with significant risk factors such as chronic recurrent stone formers with a lithogenic history, uricosuria, chronic renal failure and congenital anomalies.2,3 Encrustation may also occur in the absence of underlying urolithiasis suggesting a slow progressive phenomenon induced by urease, urinary tract infection, stasis, dehydration and long indwelling times.23 Encrustation is generally preceded by the formation of a "biofilm", which refers to the accumulation of urinary mucoprotein (slippery slime) on its surface with subsequent crystalloid deposition. Some studies have shown that hydrogel-coated stents have a higher risk of becoming encrusted in vitro than uncoated stents made of the same material.24 Spontaneous fragmentation Irrespective of the material, with the passage of time all stents are prone to ageing due to encrustation and loss of tensile strength resulting in stent fracture, breakage and even stenturia.25 Inspection of such stents has shown that these fracture lines generally pass across the stent side holes.28 The tensile elongation (maximal elongation at break point), known to be a sensitive indicator of the aging process of plastic materials, has been shown to be diminished with prolonged deployment. It is possible that the initial event may be "leaching", a dominant reaction caused by a progressive chemical urinary assault on the stent plastic and its integrity.29,30 This eventually results in fragmentation of the stent and its expulsion in urine as stenturia.31 Forgotten stent It refers to an overlooked stent32,33 that is generally associated with significant complications such as sepsis, renal decompensation, massive encrustation and stent fragmentation. Stent migration Refers to the spontaneous stent dislocation either in an upward34 or downward direction. Most polyurethane stents are suspended from the kidney with a pigtail memory at their proximal end so as to prevent migration. Migration may still occur due to the renal ureteral dynamics and peristalsis. Improper placement and incorrect size selection may contribute to stent migration. Proximal migration is most commonly due to the placement of a stent too short for the ureter.34,35 It is believed that stents must be inserted into the pelvis rather than into the calyces so as to minimize the chance of migration.36 Sepsis Sepsis associated with the presence of stents may not be specific to the stent biomaterial. Like other prostheses, DJ stents may also bind to bacteria and promote infections. Despite antibiotic prophylaxis, bio-films tend to form on the ureteric stents in vivo and bacteria tend to cling to them.37 It may be related to the degree of sterility, urinary components, and the underlying disease, and on the properties of the bacteria, especially the presence of P-fimbriae. The presence of bacteria on the stent bio-film may be of no consequence, but their colonization may be associated with urinary tract infection and sepsis. The late complications of stents (for > three months) are generally associated with increasing morbidity and an increasing frequency of encrustation, infections, secondary stone formation and obstruction of the stented tract.38 SIZE SELECTION JJ stents are available in sizes from 4.8-5-5.5-6 Fr / 16-24-26-28 cm. The most commonly used adult size is 26cm/4.8Fr. These generally admit 0.028"-0.035" guide wires. Endopyelotomy stents of 5/10,6/12 and 7/14 Fr calibre (tapering), varying in length from 24-26-28 cm are also available. The 7/14Fr size is the most commonly used endopyelotomy stent. A paediatric patient necessitates the estimation of the ureteric length and then selecting a smaller stent length such as 24/4.8 or 20/4.8. Stents of an incorrect size tend to migrate into the bladder and that may cause severe stent discomfort. STENT INSERTION & REMOVAL The usual stent assembly comprises the JJ stent, guide wire, pusher and a clip. The stent is opened under sterile aseptic conditions and assembled over a guide wire. If it is a close-ended stent the stiff end of the guide wire can be safely inserted into the leading end of the stent, the stent is then made taut over the guide wire and held in place with a clip; next, the pusher is placed over the guide wire flush with the distal end of the stent and is held in place with another clip. In case of an open-ended stent the floppy end of the guide wire should be deployed at the leading end. The assembled stent is then inserted cystoscopically (21F sheath) into the ureter under fluoroscopic guidance (retrograde stenting). As soon as the stent negotiates the distal ureter, the proximal clip is removed and the stent is advanced into the kidney by using the pusher; the distal clip is now disengaged and the guide wire is partially withdrawn until the renal coil of the stent is safely seen in the kidney. The guide wire and pusher are now gently withdrawn till the distal coil of the stent is safely seen in the bladder. Most stents have graduations on them at intervals of 5 cmthis helps in confirming precise stent placement. Alternatively, antegrade stenting39 can be performed similarly under fluoroscopic guidance through the nephroscope by sliding the stent antegradely over a pre-placed through and through guide wire, following a PCNL, when gravel is expected to choke the ureter and a tubeless PCNL is being contemplated. Most stents can be safely removed under local anaesthesia using a cystoscope with a two-pronged rigid or flexible biopsy forceps. TECHNICAL PROBLEMS Failure to negotiate the ureteric orifice This may be due to overdistension of the bladder; abnormal ureteric morphology or too rigid a stent being used. Try first placing in a guide wire through a ureteric access catheter (6F MicrovasiveTM) and then slide an open-ended stent retrogradely over it under a fluoroscopic monitor using a pusher. One may inject more lubricant into the ureteric orifice through a ureteric catheter and reattempt the stenting. Guide wire is stuck The most likely cause is an incorrect gauge of the guide wire used. Remove and reinsert, try using 0.028" guide wire in place of the 0.035" wire. Proximal coil fails to open The most likely cause is that it is in the ureter or PUJ; try pushing the guide wire, straighten the coil, advance it further and then remove the guide wire or remove and reinsert afresh. Distal coil fails to open It is most probably due to overinsertion of the stent. It may need repositioning with an ureteroscope under anaesthesia if the guide wire has been removed. Sometimes spontaneous migration may allow the distal end of the stent to pout out when it can be gently pulled out partially. MANAGING STENT COMPLICATIONS Heavily encrusted stuck stents remain one of the most challenging tasks facing the endourologist, especially when one is confronted with a long overdue forgotten stent. Multimodal endourology remains the cornerstone of management.23,40 Most mildly encrusted stuck stents respond to one or two sessions of shockwave lithotripsy.41 Those with a major proximal stone burden may need a PCNL.42 Broken stent fragments in the kidney can also be safely removed by PCNL, while ureteric fragments can be managed by minimally invasive techniques23,43-45 such as ureteroscopy and intracorporeal lithotripsy. Forgotten stents should be managed endoscopically only by those well trained and sufficiently advanced in endourology.46,47 Open surgery has a role where multimodal endourology fails, but one must remember that this is also not easy and is fraught with its own attendant risks of causing further renal impairment and sepsis. Finally, where less than 10% renal function remains, one must consider nephrectomy.23 It is important that some sort of stent diary or a computerized stent log be maintained and periodically updated by the surgeon himself so as to track overdue stents and remove them at the earliest.23,48,49 Two general strategies have been used to minimize stent encrustations associated with bacterial bio-film formation namely, use of surface-active antimicrobial-coated stents and the use of hydrophilic compounds.50 POTENTIAL RISK FACTORS FOR COMPLICATIONS Not all patients tolerate indwelling ureteral stents and some may be more prone to develop complications directly attributable to them.51 It is necessary to identify and monitor these patients more closely. Such patients should ideally either undergo an alternative form of urinary diversion or their stents should be removed /changed at the earliest. According to one study at least a third of the patients may develop one of the delayed complications.52 It is vital to recognize this high-risk group for medico-legal reasons53 as well as to prevent the occurrence of hazardous complications since this may lead to the loss of a renal unit or life. Patients with known metabolic problems, recurrent stone formers, chronically compromised renal units, congenital renal anomalies, etc. are some of the `at risk' groups. Appropriate prophylaxis should be instituted in them such as high fluid intake, timely attention to clinical complaints, aggressive treatment of documented infection and correction of metabolic aberrations with appropriate dietary and medical means. Long-term antibiotic suppression may be indicated in those with a lithogenic history on internal stenting.54 Stent malfunction can be avoided and their patency can be maintained by ensuring a high urine output through increased oral fluid intake, by prophylactic oral antibiotics and avoiding stent placement in grossly infected or bloody systems.55 NEWER EXPERIMENTAL STENTS Biodegradable stents
Valve stents
Tail stents
Dangler stents
Thermoexpandable stents
Stainless steel bead stent
PVP-coated stents
Extra-anatomic stents
Recently, antibiotic impregnated stents (adsorption of antimicrobials)61 have also hit the market. Double silver and copper-coated stents have been experimented with and they may hold the promise of keeping out sepsis (preventing bio-film formation)62 and reducing infection rates, but resistant bacteria, short leaching times and side-effects make it essential that different options be considered. Further encrustation may limit their long-term use. It is likely that surface engineered materials (hydrogels e.g. Aquavene)63 and anti-microbial drug delivery systems will be the next generation of refined stents, however, their efficacy and efficiency needs to be proven clinically.64 Hydrogel stents offer the advantage of easy placement and patient comfort.65 DURATION OF STENTING An ideal safe minimal optimal duration for stenting has not been described. No matter what the stenting duration is, all stents will form a bio-film with some degree of bacterial adherence. If left for a sufficiently long time nearly all stents will encrust. However, the safe window period of stenting is probably 6-8 weeks. Stenting following ureteroscopy or SWL for ureteric calculi is generally removed in 2-3 weeks. A difficult PCNL or ESWL associated with a risk of significant "steinstrasse" may necessitate stenting for up to 2-3 months. Patients with chronic renal failure due to obstructive uropathy or malignant ureteric obstruction may need lifelong stenting with a 3-monthly serial change. STENT MONITORING Stent monitoring includes regular monthly urine c/s analysis, serum creatinine and an X-ray KUB. Renal scans may be indicated where renal jeopardy is suspected, but these must be done with an indwelling Foleys catheter to keep the bladder empty, so as to avoid diagnosing a pseudo-obstructive pattern on the scan. Internal ureteral stent patency can be evaluated by colour-coded Doppler sonography (CCDS) or by a micturating cystourethrography.66 CCDS may have sensitivity up to 100% besides being completely non-invasive; a simultaneous KUB ultrasound scan can be done to detect any hydroureteronephrosis. To establish ureteral patency prior to stent removal, retrograde pyelography may also be attempted via the stent.67At risk stone formers should be additionally screened for metabolic abnormalities. SUGGESTED GUIDELINES & PRECAUTIONS
CONCLUSIONS Indwelling ureteral stenting should not be performed routinely. Its use must be restricted to cases where benefit overrides the complications. It is necessary that the indication for stenting, the type of stent and the size to be used be reviewed selectively. Whenever used they must be tracked closely and removed at the earliest. Late complications of stents are frequent and may appear in up to a third of the patients on long-term stenting. A closer follow-up and frequent periodic monitoring is indicated in them and in the susceptible at risk population. Appropriate prophylaxis and safety guidelines and precautions should be strictly adhered to in all cases that undergo indwelling ureteral stenting. REFERENCES
© 2003 Indian Journal of Surgery. Also available online at http://www.indianjsurg.com The following images related to this document are available:Photo images[is03080t1.jpg] [is03080t2.jpg] |
| |||||||||

{kind=link}
{kind=link}