 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 65, No. 5, Sept-Oct, 2003, pp. 413-417 The value of a joint cerebrovascular neurology clinic in carotid surgery practice D. Rittoo, H. S. Khaira,* M. Sintler, M. T. E. Heafield,** R. K. Vohra Department of Vascular Surgery and **Neurology, University Hospital Birmingham
NHS Trust, Raddlebarn Road, Selly Oak, Birmingham B29 6JD and *Consultant Surgeon,
Good Hope Hospital, Rectory Road, Sutton Coldfield, B74 2TW.
Paper Received: January 2003. Paper Accepted: March 2003. Source of Support: Nil. How to cite this article: Rittoo D, Khaira HS, Sintler M, Heafield MTE, Vohra RK. The value of a joint cerebrovascular neurology clinic in carotid surgery practice. Indian J Surg 2003;65:413-7. Code Number: is03081 ABSTRACT Objectives: The aims of the clinic were to offer suitable
patients carotid endarterectomy with minimal delay, to discuss patients with
unclear symptoms and to offer the best advice to patients referred with asymptomatic
carotid artery stenosis.
KEY WORDS: Joint clinic, Carotid endarterectomy, Stroke prevention, Transient ischaemic attack. INTRODUCTION Stroke is a cause of 12% of all deaths in England and Wales and one of the most important causes of severe disability in the United Kingdom.1 The management of patients with stroke consumes about 4.6% of the annual National Health Service budget and 6% of all hospital costs for Scotland.2 Carotid endarterectomy in patients with hemisphere or ocular transient ischaemic attacks with severe ipsilateral internal carotid artery stenosis has proven beneficial in reducing the subsequent risk of stroke.3.4 Often, there are delays in offering surgery to suitable patients. Delays of up to six months have been identified in the Vascular Surgical Society of Great Britain and Ireland audit.5 The benefit of surgery is questionable if the operation is delayed beyond six months.6 Some patients referred for investigations of possible transient ischaemic attack present with a plethora of non-specific symptoms.7-9 Involvement of a neurologist at an early stage has been shown to reduce inappropriate investigations and treatment in this group of patients.10 Often patients with non-specific symptoms and carotid bruits are referred by their general practitioner for investigations. The paucity of clinical evidence currently available on the management of such patients with asymptomatic stenosis makes adequate counselling and strict medical supervision all the more important.11,12 A clinic was set up with an access to joint consultations with a vascular surgeon and a neurologist. The aims were:
We report our experience from this clinic over a period of two years. MATERIAL AND METHODS The case notes of all the patients who attended the clinic between January 1997 and December 1998 were reviewed and a pro-forma completed. The names of all patients who underwent carotid endarterectomy during that period were cross-checked against the patients who were referred to the combined clinic. The time from referral to consultation was calculated from the date the referral letter was received by the hospital to the date the patient was seen in the clinic. The waiting time for surgical treatment was calculated from the time of the first consultation in the clinic to the date the patient underwent carotid endarterectomy. The waiting time before the joint cerebrovascular neurology clinic was established and calculated from the entries of thirty sets of notes picked at random. The number of patients who had joint consultations and the reasons for the joint consultations were noted. The number of patients who had a diagnosis and treatment plan on their first visit to the clinic was also noted. All waiting times were expressed as mean in weeks. As the waiting times were normally distributed, the means were compared using the Student t test. The result was considered statistically significant if p< 0.05. RESULTS From January 1997, 24 monthly clinics were held. One hundred
and eighteen new patients and 281 follow-up patients were seen. All new patients
had a careful history taken followed by an examination of their neurological
and cardiovascular systems. Colour Flow Doppler (CFD) was used for further
assessment of
patients with probable extracranial carotid disease.
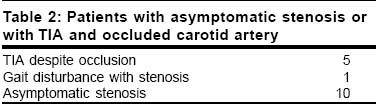
CFD Seventy-three patients were listed for carotid endarterectomy. One patient declined carotid endarterectomy despite adequate counselling. Sixty-six patients benefited from combined consultations. These patients fell broadly into two groups: (a) Patients with asymptomatic stenosis or TIA with occluded
internal carotid artery. There were 16 patients in this group (Table
2).
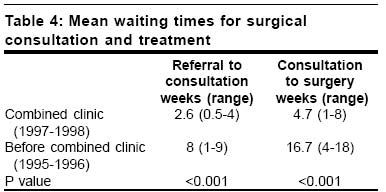
The mean waiting times from referral to outpatient consultation
and from consultation to operation were 2.6 weeks (range: 0.5-4 weeks) and
4.7 weeks (range: 1-8 weeks) respectively. Three patients required cardiology
consultations prior to surgical treatment. The mean waiting time from consultation
to operation was skewed as a result. The reduction in waiting
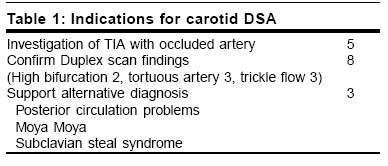
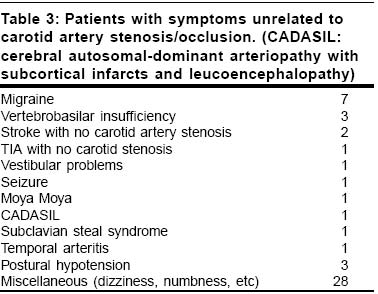
time DISCUSSION Murie et al13 and Brittenden et al,14 comparing carotid endarterectomy practice in the UK before and after publications of NASCET and ECST, found that the number of carotid endarterectomies performed was increasing. In symptomatic patients with an appropriate stenosis, carotid endarterectomy confers significant benefits in terms of stroke risk reduction. A TIA should be promptly evaluated, as delays in diagnosis and treatment increase the risk of preventable stroke.15 The risk of stroke is greatest soon after the TIA15 and in patients with cerebral TIA or with contralateral carotid artery occlusion.16,17 The evaluation of patients with TIA should therefore attempt to define the cause and determine a management plan as soon as possible after the initial event. One of the aims of the combined clinic was to offer carotid endarterectomy to suitable patients without delay. Before the cerebrovascular neurology clinic was set up, patients waited for an average 8 weeks prior to consulting a vascular surgeon and a further 16.7 weeks before undergoing carotid endarterectomy (Table 4). In the period before the establishment of the joint clnic, much of the delay in consulting a vascular surgeon probably arose from the assessment by a neurologist or a physician before referral to a vascular surgeon. The national audit of the Vascular Surgical Society of Great Britain and Ireland showed a combined morbidity and 30-day mortality of 3.4% and a postoperative stroke rate of 2.1%.5 However, as there were long delays of up to six months in offering surgery, it may be possible that some of these patients were already in the asymptomatic group at the time of surgery and therefore did not fully benefit from the treatment. Since the combined clinic was set up, we have been able to achieve a satisfactory reduction in waiting times for treatment of patients at risk of preventable strokes. The urgency of the operation was dictated by both the clinical assessment16 and the CFD findings. The availability of CFD imaging in the clinic together with the joint consultations between the neurologist and the vascular surgeon within the same clinic have both contributed towards achieving this goal (Table 4). The indication for a specific test depends on the sensitivity of the test and the management implications of a positive result, its cost and the risk to the patient. However, a minimum evaluation is desirable to exclude a diagnosis that would significantly alter management.18 Carotid Duplex ultrasonography is reported to have an accuracy of 90 to 95% but is not without limitations.19 The accuracy of ultrasonography in assessing mild to moderate stenosis is poor and total occlusion cannot always be distinguished from high-grade stenosis with trickle flow.20 The detection rate of significant stenosis in the carotid artery from indiscriminate CFD assessment is poor.21 Perkins et al reviewed 1041 new referrals for carotid Duplex scanning over a period of 18 months in Oxford and found significant disease in only 13.5%.22 Holdsworth et al in a study in the Tayside region found that 79.1% of the 1052 new scans performed were either normal or had less than 50% stenosis in one vessel.23 In the joint clinic, CFD was performed in only those patients who were likely to have extracranial carotid disease (86.4%). This allowed better channelling of existing resources, and cutting down on the number of patients awaiting investigations. Carotid DSA was used selectively when it was felt that further information about the carotid artery might alter management. Carotid DSA was performed in five patients in whom the arterial anatomy was not very clear; in another five patients for further assessment of the occluded internal carotid artery; and in one patient at the time of subclavian artery angioplasty for subclavian steal syndrome. In two patients carotid DSA was performed to establish the diagnosis of Moya Moya and evaluate presumed posterior circulation symptoms respectively (Table 1). One patient had ocular symptoms with normal carotid arteries. There were relatively few patients with asymptomatic carotid artery stenosis. In this group of patients the diagnosis was made using CFD scan. Although the ACAS11 results were generally favourable to surgical treatment, latitude from strict guidelines is generally warranted in selecting patients for endarterectomy for asymptomatic stenosis. These patients were given the best medical advice24,25 based on adjusting modifiable risk factors such as hypertension.26 In the joint clinic, over a period of two years, only five patients had symptoms of hemisphere or ocular TIA despite an occluded ipsilateral internal carotid artery. These patients pose a problem as they are at risk of further stroke and other vascular events. The source of these emboli may be from the proximal or distal stump or from plaques within the common carotid artery which find their way through collateral channels to the cerebral hemisphere. Surgically correctable problems were sought for by further assessments with carotid DSA. This small group of patients, who represent a recognised `grey area' of clinical practice, were anticoagulated following joint consultations, in view of a poor previous response to antiplatelet therapy. The assessment of patients with transient ischaemic attacks is dictated in part by the individual medical history and specific characteristics of the TIA. The goals of diagnostic tests are to identify or exclude aetiologies of TIA that require specific treatment, to assess modifiable risk factors and to determine prognosis. TIA diagnosis made by a non-neurologist can be erroneous.10,27 In this respect, consultation with a neurologist can be cost-effective by decreasing the number of inappropriate investigations.28 It has been shown that in the absence of neurological consultation, one third of all patients diagnosed with TIA will be subjected to inappropriate or inadequate investigation.10 In a regional neurovascular unit, Humphrey found that on an average only 2-3 patients out of the 25 patients referred each week were candidates for surgery. As the ratio of asymptomatic to symptomatic carotid artery stenosis is roughly 50:1 in a population of one million, the scope for inappropriate surgery is considerable.29 In the clinic, joint consultation took place if the symptoms were non-specific or if the diagnosis of cerebrovascular disease was in doubt (Table 3). Twenty-nine (24.6%) patients were assessed and discharged from the combined clinic on their first consultation. Of these patients, 13 (44.8%) had a CFD scan. The success of this combined clinic lies in there being an
adequate number of new patients to be seen every
clinic. In the first year many teething problems
were encountered until the general practitioners were
fully aware of the potential benefits for patients. This
clinic differs from one-stop clinic runs in various hospitals
in that patients are assessed not only for
extra In summary, the joint cerebrovascular neurology clinic has removed some of the obstacles that have so far denied suitable patients rapid access to an optimum assessment and carotid endarterectomy. Moreover, the combined clinic has provided an appropriate environment for the continuing care of patients who are not candidates for carotid endarterectomy. REFERENCES
© 2003 Indian Journal of Surgery. Also available online at http://www.indianjsurg.com The following images related to this document are available:Photo images[is03081t3.jpg] [is03081t4.jpg] [is03081t2.jpg] [is03081t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}