 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
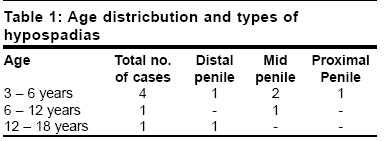
Indian Journal of Surgery, Vol. 65, No. 5, Sept-Oct, 2003, pp. 418-419 Single-stage repair of hypospadias using cremastero- tunica vaginalis pedicle flap Probhas Kumar Sarkar Department of General Surgery, I.P.G.M.E. & R. and S.S.K.M. Hospitals,
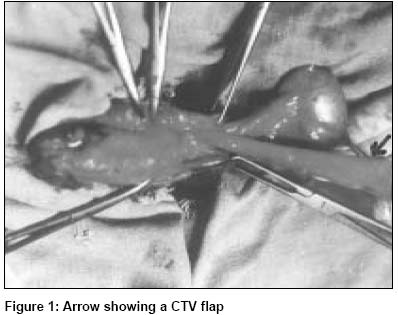
Kolkata 700020. Paper Received: July 2002. Paper Accepted: December 2002. Source of Support: Nil. How to cite this article: Sarkar PK. Single-stage repair of hypospadias using cremastero-tunica vaginalis pedicle flap. Indian J Surg 2003;65:418-9. Code Number: is03082 ABSTRACT Since the inception of the single-stage repair of hypospadias several operative techniques have been described, but have proved fullproof. Surgeons have attempted to use the dartos pedicle or tunica vaginalis as an added protective layer to prevent fistula formation, but in most cases these tissues cannot be taken up to the tip of the penis. The cremastero-tunica vaginalis (CTV) flap being longer it can be extended up to the distal end of the urethra. This series details our experience with repair of six cases of penile hypospadias of varying severity using the CTV flap. The ages of the patients varied from 3 to l8 years. Two of them had one previous failure in one patient two previous repairs had been unsuccessful. Using the CTV repair none of the patients had a fistula. A single-stage urethroplasty using a CTV pedicle flap being a promising techjnqiue merits further investigation in the treatment of a larger number of cases of hypospadias. Key Words: Hypospadias, Penile, Cremastero-tunica vaginalis pedicle flap. Hypospadias is a congenital developmental anomaly of the urethra and the penis affecting approximately 1 in 350 living male babies. Its incidence and severity seems to be on the rise. The severe form is associated more with `chordee' or a ventral bending of the penile shaft.1 The more severe the variety, the more it affects the urinary and sexual function. Thus, almost all patients with hypospadias merit surgical correction. Surgery at an early age (6-18 months) is known to give best functional results. This paper describes our experince with the use of a cremastero-tunica vaginalis flap in the repair of hypospadius. MATERIALS AND METHODS We performed this repair in six patients between October 2000 to December 2001. Table 1 shows the age distribution and type of hypospadias. One patient had two previous operations and two others had one previous operation for the correction of hypospadias. All patients were examined carefully to diagnose / exclude chordee and investigated to rule out any other congenital urological abnormality. Blood investigations and radiuological imaging were undertaklen to assess fitness for surgery. For the construction of the neo-urethra we used the tubularised incised plate (TIP) and the flip flap method. For ventral bending / chordee correction fibrolysis was performed on the sides of the urethral plate and dissection on the dorsum of the normal portion of the distal urethra.2 By this method, the penile deformity could be corrected in most patients as confirmed by intracavernous injection of normal saline. One patient needed dorsal plication of tunica albuginea. Operative procedure After making skin incision as per plan of TIP or flip flap, the penis was fully degloved down to its base, avoiding injury to the dorsal neurovascular structures. The neo-urethra was then constructed around an 8 Fr or 10 Fr catheter or an infant feeding tube. Then, the testes were accessed through the base of the degloved penis. Thereafter the tunica vaginalis of the testis was carefully mapped out and a full thickness tongue-shaped tunica vaginalis flap was created without injuring the testis or the epididymis. The tongue-shaped tunica vaginalis flap was extended along and keeping its continuity with the cremasteric muscle proximally and without injuring the vascular structure of the spermatic chord (Figure 1). The testis was replaced inside the scrotal sac and the tongue-shaped flap placed over the neo-urethra. The flap was then secured by stitching the margins with tunica albuginea on either side of the neo-urethra using 5/ 0 polyglactin sutures. The penile skin was then sutured ventrally. As tension was noticed in the penile skin, a dorsal slit was done in one patient. RESULTS The urinary catheter was removed in all patients on the 8th postoperative day. One patient had a small portion of prepucial skin necrosis, but for the others the final result was satisfactory. No patient developed a fistula. The quality of urinary flow was satisfactory in all the patients. DISCUSSION The first recorded hypospadias surgery was done in AD 100-200 by Heliodorus and Antyllus in the form of amputation of the penis distal to the distal urethral opening.3 The modern age of the repair of hypospadias began in the year 1950 with the advent of the single-stage procedure for the correction of penile deformity and the repair of hypospadias simultaneously.4 A variety of single-stage techniques are currently in use. However, many of the procedures do not produce satisfactory results in all patients. Fistula formation is the commonest cause of failure. As most of the times both the suture lines superimpose on the ventral surface, with a minimum tension there is every chance of urinary leakage and giveaway of the suture lines.5 we place an intact vascular flap over the neo-urethra and thereby urinary leakage could be prevented by the intact mesodermal layer of the CTV flap. In this series all the patients had In penile hypospadias and were treated by CTV pedicle flap. Although the creation of the CTV flap seems to be time consuming and tedious, in fact, it is quite straightforward. Although the reported series is small, this method of reconstruction merits further investigation to assess its suitability for treating patients with other types of hypospadias. REFERENCES
© 2003 Indian Journal of Surgery. Also available online at http://www.indianjsurg.com The following images related to this document are available:Photo images[is03082f1.jpg] [is03082t1.jpg] |
| |||||||||

{kind=link}
{kind=link}