 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 65, No. 5, Sept-Oct, 2003, pp. 420-422 Internal drainage of liver hydatid - concerns and solutions Gajanan D. Wagholikar, Sadiq S. Sikora, Ashok Kumar, Rajan Saxena, Vinay K. Kapoor Department of Surgical Gastroenterology, Sanjay Gandhi
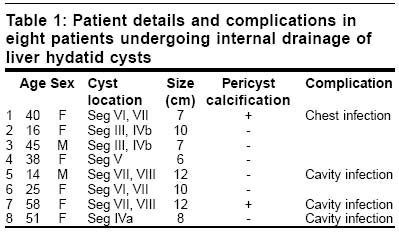
Post Paper Received: July 2002. Paper Accepted: January 2003. Source of Support: Nil. How to cite this article: Wagholikar GD, Sikora SS, Kumar A, Saxena R, Kapoor VK. Internal drainage of liver hydatid - concerns and solutions. Indian J Surg 2003;65:420-2. Code Number: is03083 ABSTRACT There are a number of procedures for the surgical management of liver hydatid and controversies still persist regarding the best technique Forty-three patients with hydatid disease of the liver were managed surgically between 1991 and 1998. Internal drainage (Roux-en-Y cysto-jejunostomy) was performed in eight cases of liver hydatid with biliary communications. Internal drainage was associated with a high incidence of the infection of the residual cavity with abscess formation (n=3/8, 38%). In all the three patients the cyst was located in the superior segments of the liver (VII, VIII, IVa). In two of the three patients the cyst was larger than 10 cm. Dependent siting of stoma is a key for the successful outcome of internal drainage in liver hydatid. This procedure is best avoided in large cysts, especially those located in the superior segments and with pericyst calcification. Key Words: Liver parasitic cyst, Cysto-jejunostomy, Surgery. INTRODUCTION Hydatid disease of the liver is a major health problem seen worldwide. The last decade has witnessed the evolution and adoption of alternative techniques of management like chemotherapy and percutaneous drainage which in selected cases are comparable to surgery. But surgery unanimously remains the mainstay of treatment and the only available modality which is applicable over the entire spectrum of the disease.1 Despite voluminous data available in the literature, controversies prevail over the preferred surgical procedure. We report our experience with internal drainage and wish to draw attention to the limitations of this procedure. MATERIAL AND METHODS Between 1991 and 1998, 43 cases of liver hydatid underwent surgical treatment at the Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow, a tertiary level health care centre. The case details and follow-up records of these patients were studied. There were 14 men and 29 women with a mean age of 34 years. Methods used for diagnosis were ultrasonography (US) and computed tomography (CT) scanning. The diagnosis was confirmed by serology, especially when imaging modalities were inconclusive. Patients were operated after a preoperative course of Albendazole (10 mg/kg for 4 weeks) to achieve sterilization and decrease the risk of recurrence in case of intraoperative spillage. The choice of operative procedure was guided by the size and the location of the cyst, and the presence of complications. RESULTS Upper abdominal pain (n=34, 79%) was the most common clinical symptom followed by a lump in the upper abdomen (n=16, 37%). The other presenting symptoms were fever (n=9, 21%), jaundice (n=4, 10%), dyspnoea (n=3, 7%) and bilioptysis (n=1, 2%). In 4 (10%) patients the diagnosis was an incidental finding at US examination performed for other reasons. Eleven patients (26%) had complicated liver hydatid cysts - 5 had infection, 4 had intrabiliary rupture and intrathoracic and intraperitoneal rupture was present in one patient each. Preoperative Endoscopic Retrograde Cholangiography (ERC) was performed in two patients with a suspicion of intrabiliary rupture. Surgical procedures performed in the management of the liver hydatid were cystopericystectomy (n=7), left lateral segmentectomy (n=2), capsulorrhaphy (n=17), internal drainage i.e. Roux_en-Y cysto-jejunostomy (n=8), omentoplasty (n=4) and external drainage (n=5). In all 4 patients with intrabiliary rupture, the common bile duct (CBD) was explored. Hydatid membranes were removed with the aid of a choledochoscope and the CBD was closed over a T-tube. There was no mortality. Postoperative morbidity
was encountered in 32% (n=14) patients. The
important complications were: wound infection - 6,
chest infection - 3, external biliary fistula - 2 and infection
of the residual cavity with suppuration
DISCUSSION There is no standard procedure for the management of liver hydatid. An individualized management and a flexible approach are the key to successful management. In the presence of significant cyst-biliary communications, repair of which carries the risk of jeopardizing biliary drainage, and / or in the presence of large calibre biliary fistulae, the cyst can be drained internally, usually by a Roux-en-Y cysto-jejunostomy. Internal drainage of the cyst into the Roux loop has been reported in a number of series as a safe and useful procedure with good results.2,3 This procedure has the dual advantage of draining the biliary communications into the digestive tract and also managing the residual cavity. Lygidakis performed this procedure in 18% of cases of intrabiliary rupture.2 Alwan performed this procedure in 10 out of 14 patients with occult biliary communication with good results in comparison to the remaining four patients who had external biliary fistulae for three to eight months following external drainage.3 Internal drainage by cysto-gastrostomy has also been recommended in case of cysts located in the left lobe of the liver.4,5 We have had a high incidence of infective complications (38%)
with this procedure with suppuration in the residual cavity which necessitated
percutaneous external drainage. The hydatid cyst in the liver is different
from other liver cysts because the cyst does not collapse after evacuation
due to the presence of the lining ectocyst. This gives rise to a residual cavity
and its incipient problems after cyst evacuation. In a study of hydatid cysts
in children who underwent evacuation, in as many as 35% of the cases the residual
cavities persisted till one year. The majority disappeared by 18 months but
in 9% they were present even after 5 years.6 Endoscopy of the cavities
in the cysts managed by wide catheter drainage has shown them to be lined by
white areolar tissue which prevents collapse.7 The above situation
is more likely to be encountered in dealing with a large cyst or with pericyst
calcification which prevents collapse of the residual cavity. If the internal
drainage is not dependent it will result in the stagnation of the contents
which in the setting of a cyst-biliary fistula will lead to infective complications.
This is the Achilles heel of this logically attractive and theoretically sound
procedure. In such clinical situations other appropriate surgical options (i.e.
excision, omentoplasty) are to be exercised to deal with the residual cavity.
In all the three patients with suppuration reported in the present study, the
cyst was located in the superior segments. In two of these patients the cyst
was more than 10 cm We conclude by emphasizing that for a successful internal drainage it is essential to elect a case carefully, the important considerations being: a. Site: Cysts located in the superior segments (VII, VIII and IVa) should not be drained internally as far as possible as it is difficult to do a dependent cysto-jejunostomy due to their location. b. Size: Large hydatid cysts can give rise to the problem of a persistent residual cavity, especially in the presence of pericyst calcification. Finally, one should always ensure a dependent stoma placement as non-dependent drainage will give rise to a "tea pot" effect which is a sure recipe for "brewing" infective complications in the residual cavity. REFERENCES
© 2003 Indian Journal of Surgery. Also available online at http://www.indianjsurg.com The following images related to this document are available:Photo images[is03083t1.jpg] |
| |||||||||

{kind=link}