 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 65, No. 5, Sept-Oct, 2003, pp. 423-426 Spontaneous pneumothorax A. G. Ahangar, Shah Shabir Hussain, Ishtyak Ahmad Mir, Abdul Majid Dar, Mohd. Akbar Bhat, Ghularn Nabi Lone, Rauf Ahmad Wani, Mohd. Afzal-u-din Department of Cardiovascular and Thoracic Surgery, Sher-i-Kashmir Institute
of Medical Sciences Srinagar, India Paper Received: October 2002. Paper Accepted: July 2003. Source of Support: Nil. How to cite this article: Ahangar AG, Hussain SS, Mir IA, Dar AM, Bhat MK, Lone GN, et al. Spontaneous pneumothorax. Indian J Surg 2003;65:423-6. Code Number: is03084 ABSTRACT Background: Spontaneous pneumothorax is classified
into primary spontaneous pneumothorax (PSP) and secondary spontaneous pneumothorax
(SSP). PSP occurs without any cause, usually as a result of the rupture of
subpleural blebs. SSP is related to the presence of underlying lung disease.
The pathological consequences depend primarily on the site of pneumothorax
and the condition of the underlying lung.
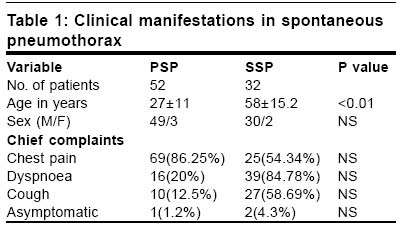
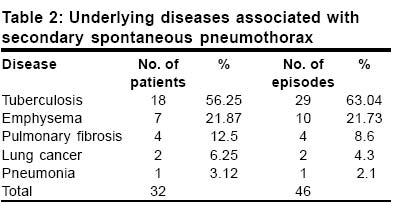
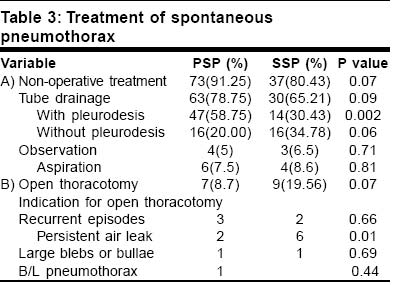
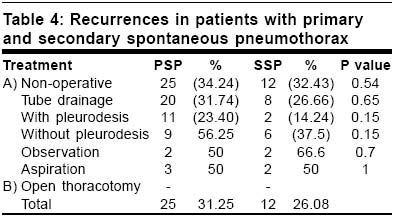
Key Words: Spontaneous pneumothorax, Therapy. INTRODUCTION Pneumothorax is the accumulation of air within the pleural space. Spontaneous pneumothorax (SP) is classified into primary spontaneous pneumothorax (PSP) and secondary spontaneous pneumothorax (SSP). PSP occurs without any cause, usually as a result of the rupture of subpleural blebs.1,2 SSP is related to the presence of underlying lung disease. The pathological consequences depend primarily on the site of pneumothorax and the condition of the underlying lung.The purpose of this study is to describe the clinical manifestations and to assess different modalities of treatment, especially the role of open thoracotomy in SP. MATERIAL AND METHODS The medical records of 82 patients with 126 episodes of SP, treated at Sher-I-Kashmir Institute of Medical Sciences from January 1998 to December 2000 were reviewed for this study. Patients with traumatic and iatrogenic pneumothorax were excluded from the study. Patients with obvious cause of pneumothorax were categorized as SSP. The results of PSP were compared with SSP. The patients were followed up on an OPD basis. Statistical analysis was done using x2 test and continuous data were compared by Student's test. RESULTS The age of patients with PSP was 27±11 years and for SSP 58.8±15.2 years (p<0.01). Eighty-nine (94.23%) patients of PSP were males and 3 (5.76%) were females. Among SSP patients, there were 30 (93.75%) males and 2 (6.25%) females. Clinical manifestations The clinical manifestations are summarized in Table 1. Pain was the commonest symptom with PSP episodes (86.25% PSP vs. 54.34% SSP) whereas dyspnoea was the most common feature of SSP episodes (20% PSP vs. 84.78% SSP). There was one patient (1.25%) of PSP who was asymptomatic in comparison to 2 patients (4.3%) of SSP. Aetiology The commonest underlying cause of SSP was tuberculosis (Table 2). Twenty-nine episodes (63.04%) in 18 patients (56.25%) occurred with this disease. Ten episodes (21.73%) in 7 patients (21.87%) were due to emphysema. Pulmonary fibrosis, lung cancer and pneumonia were responsible for 4, 2 and 1 episodes respectively. Treatment Nonoperative treatment: The commonest mode of treatment was tube thoracostomy for both groups of patients (Table 3). Sixty-three (78.75%) episodes of PSP were managed with tube thoracostomy in comparison with 30 episodes (65.21%) of SSP (30.43%). Pleurodesis was performed in 47 episodes (58.75%) of PSP in comparison to 14 episodes (3043%) of SSP. Other non-operative modes of management were needle aspiration (8.7% in PSP vs. 19.56% in SSP) and observation (5% in PSP vs. 6.5% in SSP). Operation (Table 3) Seven episodes (8.7%) of PSP had open thoracotomy as compared to 9 (19.5%) episodes of SSP. The commonest indication for surgery in PSP was recurrent episodes whereas the commonest indication in SSP was persistent air leak. Open thoracotomy through the posterolateral approach was used for all the patients. All 7 patients of PSP were managed by excision of blebs and bullae with oversewing of area and pleural abrasion. Patients with SSP were managed by lobectomy in 4 and pneumectomy in 1 episode. Excision of bullae with oversewing of area with pleural abrasion and pleurectomy was done in 2 episodes each. Recurrence (Table 4) The overall recurrence rate for both groups of patients was higher with non-operative treatment (34.24% in PSP vs. 26.08% in SSP). There were no recurrence rates with operative treatment in both groups of patients. DISCUSSION Pneumothorax is the accumulation of air within the pleural space. PSP occurs in young patients without any apparent lung disease. SP with underlying lung disease is categorized as SSP. A pneumothorax compresses lung tissue and reduces pulmonary compliance, ventilatory volumes and diffusing capacity. Patients with SP present with chest pain and dyspnoea. Less common symptoms include non-productive cough and orthopnoea. Rarely, patients may be asymptomatic. In our series chest pain was the commonest symptom of PSP (86.25% in PSP vs. 54.34% in SSP) and dyspnoea was the commonest manifestation of SSP (20% in PSP vs. 84.78% in SSP). Tanaka et al3 reported dyspnoea in 64.24% patients with SSP and in 10.2% patients with PSP. They also reported chest pain as the commonest manifestation in PSP in comparison to SSP (88.16% in PSP vs. 39.8% in SSP). The occurrence of apical blebs and bullae in patients with PSP has been found to be greater than 85% in most recent surgical series.1,2 The most common underlying lung disease in our series of patients with SSP was tuberculosis, 29 episodes (63.04%) in 18 patients (56.25%) followed by emphysema, 10 episodes (21.73%) in 7 patients (21.87%). The commonest cause of SSP, as per literature, goes in favour of emphysema.4,5 Getz and Beasley6 reported only 10.7% of SSP due to tuberculosis. This suggests that pulmonary tuberculosis is very common in our country. Simple needle aspiration of a pneumothorax may relieve symptoms and can promote quicker lung re-expansion.1 It may also help to determine whether the initial fistula that caused the pneumothorax has sealed or whether there is an ongoing air leak that requires chest tube insertion. Tube thoracostomy and underwater seal drainage are the mainstays of treatment for SP. Full re-expansion of the lung, even in the presence of a continuous leak, can be achieved usually with the application of suction to the thoracostomy drainage systems. In our series, most of the episodes of SP were managed by non-operative treatment. Non-operative treatment included tube thoracostomy (78.75% in PSP vs. 65.21 % in SSP) with or without pleurodesis, observation (5.5% in PSP vs. 6.5% in SSP) and needle aspiration (7.5% in PSP vs. 8.6% in SSP). Shields and Oilschlager5 reported observation in 11.7%, needle aspiration in 6.7% and thoracostomy tube drainage in 65.0% patients with SSP. In a series reported by Tanaka et al,3 60.6% episodes of PSP and 80.5% episodes of SSP were managed with non-operative treatment. Non-operative treatment included tube thoracostomy with or without pleurodesis (32.7% in PSP vs. 63.4% in SSP), observation (23.2% in PSP vs. 8.1% in SSP) and needle aspiration (4.7% in PSP vs. 8.9% vs. in SSP). The first line of treatment of SP depends on the size of pneumothorax, associated symptoms and underlying pulmonary disease. In patients with SSP, who are usually older than patients with PSP and also have diminished lung function because of underlying lung diseases, even a small pneumothorax can produce severe respiratory distress.7 Patients with small pneumothorax (<20%) who are asymptomatic or have few symptoms can be observed. Indications for intervention include progressive pneumothorax, delayed pulmonary expansion or development of symptoms. The risk of recurrent pneumothorax varies widely in published reports because of the varying age and associated lung disease. DeVries and Wolfe8 estimated a recurrence rate of 32% with non-operative methods. Granke and coworkers9 reported a recurrence rate of 22.4% with tube drainage and no recurrences in the operative group of 78 patients. Seremetis10 reported a recurrence rate of 49% with observation, 38% with tube drainage and no recurrence after open thoracotomy. Schoenenberger and coworkers11 reported recurrence rates of 30% in both PSP and SSP. Tanaka et al reported an overall recurrence rate of 28.3% in PSP vs. 30.9% in SSP.3 Their recurrence rate with non-operative treatment was 44.8% in PSP vs. 35.4% in SSP, and with open thoracotomy 3.0% in PSP vs. 12.5% in SSP. Thus, the recurrence rates observed in our series, 31.24% in PSP vs. 26.68% in SSP are comparable with figures seen in other series. To prevent recurrence, the diseased site should be resected and pleural space obliterated. Surgery for PSP has evolved over recent years from open thoracotomy (axillary or posterolateral) to a minimally invasive video-assisted approach.12,13 The surgery carried out is identical, despite the differences in approach. Apical blebs are resected. The parietal pleura over the apex of the hemithorax can be removed (pleurectomy), abraded (mechanical pleurodesis) or treated with talc or tetracycline agents (chemical pleurodesis). The recurrence rate for these procedures, performed open or closed, is less than 5%. Naunheim and colleagues14 reported a recurrence rate of 4% with VATS blebectomy and pleurodesis. They found a reduced drainage time and complication rate and a shorter hospital stay with this approach. Patients also had a high acceptance rate with this procedure. CONCLUSION Clinical manifestations and treatment options for primary and secondary spontaneous pneumothorax are similar. However, patients with SSP, generally, are debilitated from a respiratory standpoint and may have other significant comorbid diseases. Effective treatment must be individualized, but should include chemical or surgical pleurodesis in combination with complete lung re-expansion and effective sealing of air leaks. REFERENCES
© 2003 Indian Journal of Surgery. Also available online at http://www.indianjsurg.com The following images related to this document are available:Photo images[is03084t4.jpg] [is03084t2.jpg] [is03084t3.jpg] [is03084t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}