 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 65, No. 5, Sept-Oct, 2003, pp. 427-429 Radiofrequency surgery in pilonidal sinus Pravin J. Gupta Gupta Nursing Home, D/9, Laxminagar, Nagpur 440022.
Paper Received: January 2002. Paper Accepted: October 2002. Source of Support: Nil. How to cite this article: Gupta PJ. Radiofrequency surgery in pilonidal sinus. Indian J Surg 2003;65:427-9. Code Number: is03085 ABSTRACT Background: With the uncertainty about the aetiology
and the complexities encountered in treatment, pilonidal disease has been considered
as a tricky pathology. While many varieties of approaches ranging from conservative
treatment to an extensive surgical excision are in vogue, a method of laying
open of pilonidal sinus is still considered the most favoured one.
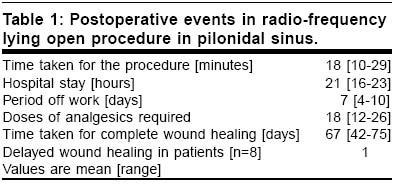
Key Words: Pilonidal sinus, Laying open, Radiofrequency surgery, Recurrence. INTRODUCTION Pilonidal sinus is a disabling disease in young adults, which can result in an abscess or draining sinus tracts, leading to long-term loss of productive capacity and it tends to have high morbidity. It probably results from hair penetration beneath the skin. Despite surgical therapy dating back to more than a century, management of this condition remains controversial. Many different approaches ranging from conservative treatment1 to extensive surgical excision have been put forth but the method of simple lying open of the pilonidal sinuses is considered as the gold standard. The procedure of sinotomy involves incision with local excision of the midline pits, extending into the central cavity and laying open lateral tracts. In this report we describe our early experience of using radiofrequency device for performing the sinotomy procedure. MATERIAL AND METHODS Eight patients of chronic pilonidal sinus were treated with the technique of radiosurgery. There were 6 males and 2 females in the age group of 16 to 35. All of them received written explanations of the technique clearly mentioning it as a new one with potential drawbacks like relapses and the need for repetition. An informed consent was obtained before the procedure. The procedure was approved by the ethical committee. Radiofrequency surgery Radiofrequency surgery is the method of cutting and /or coagulation of tissues, using a high frequency alternating current. The effect of cutting, known as high frequency section, is executed without pressuring or crushing the tissue cells. This results from the heat produced by the tissue resistance to the passage of a high frequency current. The heat makes the intracellular water boil, increasing the inner pressure of the cell to a point of breaking it from inside to outside [explosion]. This phenomenon is called cellular volatilization.2 A 4 MHZ Ellman dual frequency unit [Ellman International, Hewlett, N.Y] was used for this purpose. This instrument produces an electromagnetic wave of a very high frequency that reaches up to 4 megahertz. The unit is supplied with a handle to which different interchangeable electrodes can be attached as per the requirement. In this study, a ball electrode for coagulation, a round loop electrode for shaving the offending tissue and a fine needle electrode to open up the sinus tracts were used. Procedure A sinogram was performed to trace the length and extension of the tracts and to rule out any connection of the sinuses with the ano-rectum. The procedures were performed under spinal anaesthesia with the patient lying in the left lateral position. Methylene blue mixed with hydrogen peroxide was injected in one of the sinuses to give a guideline about the tract and branching. A probe was inserted in the tract and with the help of the fine needle electrode the tract was opened over it. When there were multiple openings, an elliptical incision was made to include all the external openings in it. The brisk bleeding encountered was controlled by holding the tissue in a haemostat and coagulating with the ball electrode. All the hair and foreign material were removed. The complete course of the tract was traced and the infected, hard tissue was shaved off with the round loop electrode leaving behind a red, raw area. Care was taken that the wound acquired a shape of an inverted cone, widest externally and narrowest internally. This prevented premature closure of the external skin wound. The procedure was swift, simple and easy to perform. As the bleeding points were coagulated during the dissection with the device, the need to ligate any bleeders was obviated, making it a `sutureless' wound. The wound was covered with an adhesive dressing. As no packing was done, the consequent discomfort created was avoided. The patients were discharged the next morning. Postoperative care The patients were advised to clean the wound with soap twice a day and apply an antiseptic ointment. A course of antibiotics and anti-inflammatory analgesics was given for the first 10 days according to the departmental protocol. The patients were followed up every two weeks in the initial period and then once a week. This schedule was observed to watch for any possibility of premature approximation of the skin before the wound underneath could heal. In such a situation, the external skin edges could be trimmed all around to keep the internal wound exposed. The aim was to allow the wound to heal from within outward. RESULTS The results are shown in table 1. The number of sinuses in each patient ranged from 1 to 3 with a mean of 2. Most of them were placed on either side of the sacrum. Discharge from the sinus and pain were the two main complaints. In one patient, delayed wound healing was faced due to early closure of the external wound requiring trimming of the edges. The wound healed uneventfully thereafter. A follow-up after 12 to 15 months did not show recurrence in any of the patients. No major complications were encountered. The minor ones encountered are deep dissection causing more scarring and longer time for healing and oedema in the surrounding tissue if power of the radio-frequency surgical unit was kept on the higher side. Two of our patients compalined of excessive discharge from the open wound. We attribute this to greater destruction of the tissues at the base and at the periphery by the radio-surgical device. DISCUSSION It has been observed that simple surgical procedures in pilonidal disease are far better than the a complex procedures if general patient satisfaction, the period of hospitalisation and the recurrence rate are considered.3-5 The ideal treatment of pilonidal sinus should be one which results in a reduced number of complications with a minimal time off work and a low risk of recurrence.6,7 The radiofrequency procedure of incision and lying open practised by us is found to fulfill these criteria. It uses a high-frequency [4MHz] radio wave instead of heat to cut and coagulate tissues. This certainly is a distinctive feature of the equipment that does away with the burning effect that is common with traditional electro-surgical devices and cautery equipment. The radio waves can be used to seal small blood vessels without creating any char, whereas the cautery or elcetro-surgical instruments create heat at the tip of the instruments to seal the affected portion with transferred heat, which invariably damages the adjacent healthy tissues.8 Radio-frequency allows the surgeon to work in direct proximity to the functional tissues that need to be preserved, like the post-sacral fascia. Incision and lying open of the sinuses by radio-frequency could be done as a day care procedure. There is less tissue trauma, pain and inflammation and the patient can return to his routine within a short duration of time. Presence of hair in the wound is one of the prime causes of incomplete healing or recurrence. The hair should be meticulously shaved at interval. Care should be taken that the wound remains free of hair all the time. A follow-up of 12-15 months was found sufficient as most `recurrences' occur within 6 months. They denote failure of treatment rather than true recurrence.9 Late recurrences after a year are less common. There is evidence to suggest that these are new sinuses and are not related to the previous treatment. CONCLUSION The ideal treatment for pilonidal sinus is one which aims at reducing hospital stay, minimizing tissue destruction by avoiding unduly extensive procedures and the resultant complications, early resumption of work by the patient while preventing recurrence. In this small series of patients, the laying open technique of pilonidal sinus using a radiofrequency device has shown encouraging results meeting most of the above criteria and this method merits further investigation. REFERENCES
© 2003 Indian Journal of Surgery. Also available online at http://www.indianjsurg.com The following images related to this document are available:Photo images[is03085t1.jpg] |
| |||||||||

{kind=link}