 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 65, No. 5, Sept-Oct, 2003, pp. 430-434 Management of nonpalpable testis: laparoscopic approach Ketan D. Mehta, Sameer M. Kacheriwala, Yogesh R. Jain, Biju S. Pillai, Ajay P. Sodhi, Vimal B. Vyas Department of Surgery, M. P. Shah Medical College, Jamnagar, Gujarat 361008. Paper Received: March 2003. Paper Accepted: May 2003. Source of Support: Nil. How to cite this article: Mehta KD, Kacheriwala SM, Jain YR, Pillai BS, Sodhi AP, Vyas VB. Management of nonpalpable testis: Laparoscopic approach. Indian J Surg 2003;65:430-4. Code Number: is03086 ABSTRACT Objective: In the present study, we investigated the
usefulness of laparoscopy in the diagnosis and treatment of nonpalpable testis.
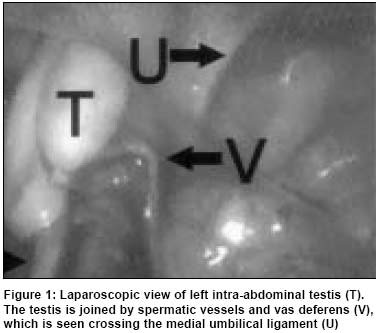
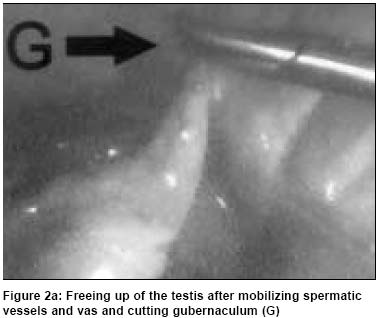
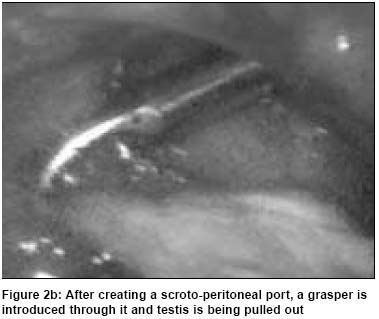
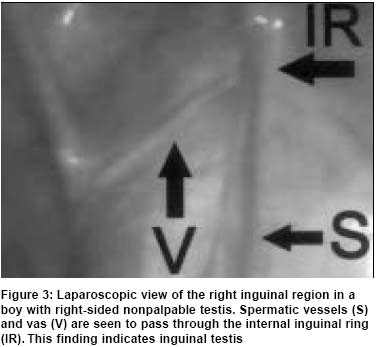
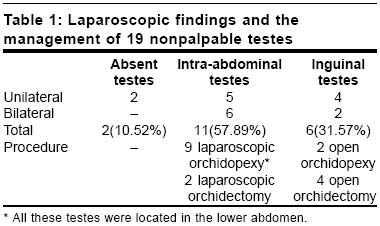
Key Words: Laparoscopy, Nonpalpable testis, Impalpable testis, Undescended testis, Cryptorchidism. INTRODUCTION Undescended testis or cryptorchidism is a common genital problem in boys. Its incidence in premature newborns is 30% and in full-term newborns is 4%.1 Nonpalpable testis (NPT) represents 25% of all undescended testes.2 NPT may be due to the vanishing testis syndrome, intra-abdominal position, examination obscured by obesity or scar tissue, and rarely due to testicular agenesis.3 NPT poses a diagnostic and therapeutic challenge to the surgeon. Given the potential of these gonads to undergo malignant transformation and causing infertility, it is essential to determine their presence or absence. Radiological imaging and open surgical exploration have proved to be unreliable in detecting it.4 Laparoscopy has become an important diagnostic modality for NPT and has also been applied in the treatment of this disease.5 Here we present a prospective study reporting our experience with laparoscopy in the diagnosis and treatment of NPT. MATERIAL AND METHODS Between January 2002 and December 2002, 15 boys with 19 NPT, aged 2 to14 years, underwent laparoscopy in a single surgical unit at our institute. Out of the15 patients, 11 had unilateral (6 left-sided, 5 right-sided) and 4 had bilateral NPT. The testis was considered nonpalpable after thorough clinical examination, ultrasonography and examination under anaesthesia failed to detect it. Diagnostic laparoscopy was performed under general anaesthesia. The abdomen was insufflated with carbon dioxide using a Veress needle, which was inserted through a small transverse skin incision placed over the superior edge of the umbilicus (pressure limit 10 mm Hg). The peritoneal cavity was examined using either a 7-mm or a 10-mm laparoscope. The inguinal region of the normal side was inspected first, followed by the inspection of the diseased side to identify the location of the spermatic vessels, vas deferens and testis. Based on the laparoscopic findings, the testes were classified into 3 groups: Group 1: Absent testes or vanishing testes: here spermatic vessels and vas deferens were ending blindly. In these patients, the procedure was terminated. Group 2: Intra-abdominal testes (Figure 1): in these cases laparoscopic orchidopexy or orchidectomy was carried out after placing additional working ports. The decision to perform orchidopexy or orchidectomy was based on the size of the testis, age of the patient and whether the condition was unilateral or bilateral. Laparoscopic orchidectomy was accomplished by ligating the spermatic vessels and vas deferens with the help of two 5-mm abdominal ports and by removing the testis through one of them. In case of laparoscopic orchidopexy, after placing two 5-mm ports, the spermatic vessels and vas deferens were mobilised by incising the peritoneum covering them. The testis was freed up by dividing the gubernaculum from its distal attachments (Figure 2a). The adequacy of mobilisation of the testis was tested intra-abdominally by ensuring that it reached the opposite internal inguinal ring. Then a `scroto-peritoneal' port was created. A grasper inserted from one of the working ports was passed from inside the internal inguinal ring traversing the inguinal canal and was made to indent the scrotal skin. A small transverse skin incision was made over the tip of the grasper indenting the scrotal skin, a dartos pouch was created and then the tip of the grasper was made to emerge through the incision. A 5-mm cannula was then loaded in a retrograde manner over this grasper into the abdominal cavity under direct vision. A grasper was next introduced into the peritoneal cavity from the scrotal side of the port to grasp the gubernaculum and draw the testis into the dartos pouch (Figure 2b). When patent processus vaginalis was found, it was occluded by placing one or two stitches of polyglactin at its neck (Figure 2c). Group 3: Inguinal testes (Figure 3): Here the spermatic vessels and vas deferens were seen entering the internal inguinal ring. In these cases, the inguinal canal was explored by a groin incision. Orchidopexy or orchidectomy was done based on the same criteria applied for intra-abdominal testes. RESULTS We encountered no complications with laparoscopy. Laparoscopic findings and the management of the 19 NPT is summarised in Table 1. Two (10.5%) testes were absent. Unnecessary extensive inguinal exploration and / or laparotomy were avoided in these cases. Eleven (57.89%) testes were intra-abdominal. Out of these, 2 (10.52%) testes were removed laparoscopically. The remaining 9 (47.36%) underwent single-stage laparoscopic orchidopexy. All the procedures were concluded successfully, without any undue tension over the cord structures. Laparoscopy has allowed wide mobilization of cord structures under a magnified view. Again, in all these cases extensive inguinal exploration and/or laparotomy were avoided. The average hospital stay of the patients was 36 hours. Six (31.57%) testes were found in the inguinal canal, which were not detected by thorough clinical examination, ultrasonography and examination under anaesthesia. But laparoscopy revealed the location of the testes. In all these cases, traditional inguinal exploration was carried out by groin incision. Four (21.05%) testes were removed and orchidopexy was performed in the remaining 2 (10.52%). DISCUSSION NPT presents a unique diagnostic and therapeutic problem. Its presence or absence must be verified and appropriate therapy should be applied to either make it palpable or to remove it. A variety of tests are employed in clinical practice to search for NPT. These include herniography, ultrasonography, CT scan, Magnetic Resonance Imaging (MRI), testicular angiography or venography.6 The more popular modes that are discussed today are ultrasonography, CT scan and MRI. Ultrasound may not be reliable if the NPT is located underneath the aponeurosis of the external oblique muscle or inside the abdomen.7 CT scan may be useful in documenting the location of the NPT but the test is expensive, emits radiation and sometimes is difficult to perform in a young child.8-11 MRI may be helpful in locating the NPT, but like CT scan it may be difficult to perform in a young child, is very expensive and is not widely available. Each of these modalities carries low false positive rate, that is, if a testis is defined on their study, usually it can be confirmed surgically. However, if a testis is not identified, one cannot safely presume its absence, since each of these modalities has a relatively high false negative rate.12 Therefore, regarding radiological evaluation of NPT, ultrasonography, CT scan and MRI cannot definitely diagnose the absence of testis. Surgical exploration to whatever extent is necessary. The reasons for correcting NPT are (1) to enhance the possibility of future fertility, (2) to place the testis at a site where it can be easily palpated because such a testis has an increased susceptibility to malignant degeneration, (3) to prevent or alleviate certain psychological tendencies and (4) to permanently correct the defect that is obvious to both the parents and the patient.6 The traditional approach to NPT has been to begin with an exploration of the inguinal canal followed by retroperitoneal or peritoneal exploration, if no testis or cord structures could be found in the inguinal canal. This approach often involves unnecessary and sometimes very extensive surgery. The advent of laparoscopy has allowed a minimally invasive approach for locating NPT. Laparoscopy is a sensitive and specific diagnostic modality for NPT and the accuracy of laparoscopy in locating a testis or proving its absence exceeds 95%.13 Laparoscopic findings define the subsequent operative steps, which may take advantage of laparoscopic access. The NPT visualised at laparoscopy is managed depending on its size, location and the age of the patient. When blind ending cord structures are visualized, no further investigation is required; the likely cause of absent testis is a prenatal or perinatal vascular accident.13 Intra-abdominal testis can be managed by laparoscopic orchidopexy or orchidectomy. The decision regarding salvage or removal is a difficult one. A small hypoplastic testis, a testis with significant ductal system abnormality or unilateral abdominal cryptorchidism in a post-pubertal patient is a poor candidate for salvage. Low intra-abdominal testis can be mobilized with laparoscopic dissection of the spermatic vessels and vas deferens and delivered to a scrotal position without dividing the spermatic vessels, as a single-stage procedure. High intra-abdominal testis can be managed either by laparoscopic one or two-stage Fowler-Stephen orchidopexy, laparoscopy-assisted testicular microsurgical autotransplantation or by orchidectomy in unilateral disease. The choice of procedure depends on individual preference and availability of expertise. If cord structures traverse the internal inguinal ring, there may be blind ending cord structures in the canal, a hypoplastic or dysplastic testis in the canal or an ectopic testis that was not palpable preoperatively. It is probable that some of these inguinal gonads that were nonpalpable preoperatively may have indeed been intra-abdominal, however, with insufflation and increased intra-abdominal pressure, they may have been forced through an open internal inguinal ring into the inguinal canal.12 There is some controversy today as to whether the inguinal canal should be explored in a patient with NPT in whom the cord structures entering the internal inguinal ring are encountered at laparoscopy.12 We believe that this situation warrants inguinal exploration as a dysplastic testis, an ectopic testis or a testis displaced from the abdominal cavity due to the increased intra-abdominal pressure caused by insufflation may be occasionally discovered. The exploration can be expeditiously performed through a small inguinal incision. CONCLUSION Laparoscopy is an excellent, low-risk, high-yield diagnostic and therapeutic tool in the management of nonpalpable testis, provided the surgeon is experienced and comfortable with the technique. We recommend its routine use in the diagnosis and treatment of this disorder. REFERENCES
© 2003 Indian Journal of Surgery. Also available online at http://www.indianjsurg.com The following images related to this document are available:Photo images[is03086f2c.jpg] [is03086f2b.jpg] [is03086f1.jpg] [is03086t1.jpg] [is03086f3.jpg] [is03086f2a.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}