 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 65, No. 5, Sept-Oct, 2003, pp. 435-436 Case Report Chondroma of the tongue Deepak Kumar Sinha, Jeevan Lal Sahni,* Asha Agarawal** Department of Cardio-thoracic & Vascular surgery, St. John's Medical College & Hospital,
Bangalore, India; *Department of Cardio-thoracic & Vascular surgery, L.P.S.
Institute of Cardiology, Kanpur, G.S.V.M. Medical College, Kanpur, India and
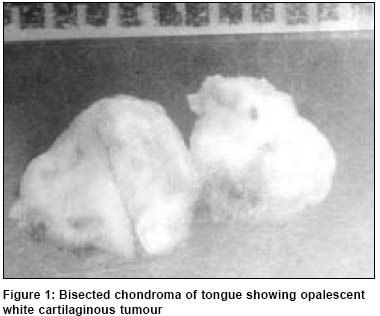
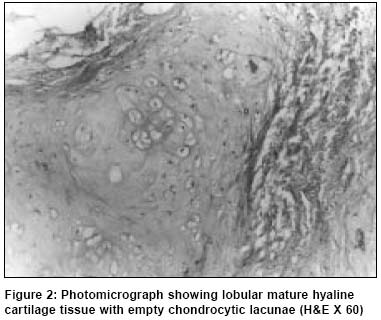
**Department of Pathology, G.S.V.M. Medical College, Kanpur, India. Paper Received: June 2002. Paper Accepted: October 2002. Source of Support: Nil How to cite this article: Sinha DK, Sahni JL, Agarawal A. Chondroma of the tongue. Indian J Surg 2003;65:435-6. Code Number: is03087 ABSTRACT The occurrence of chondroma in the soft tissue of the oral cavity is uncommon. This anomaly occurs mainly on the lateral side or dorsum of the tongue. Here we report a case of a well-defined cartilaginous tumour of the tongue in a 10-year-old boy, diagnosed histologically as a chondroma. The swelling was present on the dorsal aspect of the right half of the tongue at the junction of its posterior 1/3 and anterior 2/3. The swelling was removed successfully in toto and the patient made an uneventful recovery. Key Words: Tongue, Chondroma. INTRODUCTION Chondroma is a benign neoplasm derived from mesodermal cells that form cartilage. Chondromas are commonly seen in short tubular bones and flat bones. Rarely, they may arise in soft tissue as a hamartomas, but their occurrence in the tongue is extremely rare.1,2 CASE REPORT A 10-year-old boy presented with a slowly growing swelling over the tongue of 8 years duration. He did not complain of any pain in the swelling. Examination revealed a smooth, firm, non-tender, and slightly mobile swelling measuring 2.5 X 2 cm on the right half of the tongue at the junction of its posterior 1/3 and anterior 2/3. There was no cervical or submental lymph node enlargement. At surgery the swelling could be removed in toto with ease via a longitudinal incision over the tongue. Gross examination of the excised swelling revealed a globular, well-encapsulated greyish brown, mass with greyish white cut surface (Figure 1). Microscopy showed a well-encapsulated tumour with lobules of mature hyaline cartilage, having several well-formed chondrocytes embedded in the myxo-hyaline matrix. Many of the chondrocytes had a single nucleus. No mitosis was observed (Figure 2). Based on these findings a histopathological diagnosis of chondroma of the tongue was made. The patient was discharged the day after surgery and remains well a year later. DISCUSSION Chondromas are benign tumours of bone, characterised by proliferating mature chondrocyte lying in a hyaline myxoid matrix. Various terms such as chondroma, cartilaginous choristoma, osteocartilaginous choristoma, osteochondroma and chondroma with ossification or calcification have been used by different authors to refer to tumours of the tongue with similar histological findings. In tongue these tumours probably arise as a result of cartilaginous differentiation of undifferentiated mesenchymal cells. The theories of origin of this glossal lesion relate to either ectopic embryonic rests of pleuripotent mesenchyme or post-traumatic mesenchyme metaplasia.3,4 These lesions are usually located in the middle third of the dorsum of the tongue5 but they have also been reported in the buccal mucosa, soft palate6 and in the neck associated with a branchial cleft cyst.7 It has been stated that chondromas which occur at the antero-lateral region of the tongue may be traumatic in origin since this site is more vulnerable to trauma.1 Cartilaginous rests are the origin of lingual chondroma on the dorsum of the tongue.8 Immunohistochemistry confirmed the lesion to be mesenchymal and not epithelial in origin. In the differential diagnosis it is important to exclude chondromatous change in a pleomorphic adenoma and also the possibility of a metastasis from an osseous chondrosarcoma. In our patients the tumour presented well-formed lobules of hyaline cartilage containing proliferating mature chondrocytes. As in our patient, the tumour can usually be successfully removed in toto without leaving behind any residual disease. Carbon dioxide laser facilitates the excision, providing a dry surgical field. It is important to bear in mind this rare tumour when presented with a swelling in the tongue and treat it adequately by surgical removal. REFERENCES
© 2003 Indian Journal of Surgery. Also available online at http://www.indianjsurg.com The following images related to this document are available:Photo images[is03087f1.jpg] [is03087f2.jpg] |
| |||||||||

{kind=link}
{kind=link}