 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 65, No. 5, Sept-Oct, 2003, pp. 436-438 Case Report Ganglioneuroma of the adrenal gland Daljeet Singh, Amreek Singh, B. R. Prabhakar, Raman Arora, Satish Jain, G. S. Hara, Lovneesh Garg, R. S. Sibia Department of Surgery, Mohan Dai Oswal Cancer Treatment & Research Foundation,
Ludhiana, Punjab.
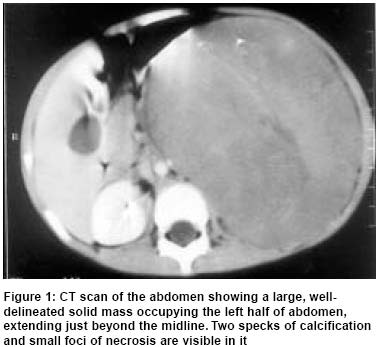
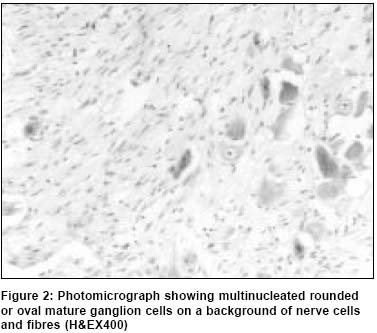
Paper Received: April 2002. Paper Accepted: June 2002. Source of Support: Nil. How to cite this article: Singh D, Singh A, Prabhakar BR, Arora R, Jain S, Hara GS, et al. Ganglioneuroma of the adrenal gland. Indian J Surg 2003;65:436-8. ABSTRACT Ganglioneuromas are rare, benign, well-differentiated tumours of the primordial neural crest, majority of which occur in older children and adults. We report a rare case of ganglioneuroma of the adrenal gland occurring in a four-year-old child and discuss its clinical presentation, histological features and various diagnostic modalities. Key Words: Adrenal, Ganglioneuroma, Neuroblastoma. INTRODUCTION Ganglioneuromas are rare, benign, well-differentiated tumours of the primordial neural crest. The majority of these tumours occur in older children and adults. These tumours are most often located in the posterior mediastinum and the retroperitoneum but only a small proportion are localized in the adrenal gland. We report a rare case of ganglioneuroma of the adrenal gland occurring in a four-year-old child and discuss its clinical presentation, histological features and various diagnostic modalities. CASE REPORT A 4-year-old girl presented to us with a mass in the left side of abdomen of 15 days duration. On examination the patient was normotensive; a large, bimanually palpable mass occupying almost the whole of the left side of the abdomen was present. The haematological and biochemical parameters were within the normal range. X-ray of the chest was normal. CT scan revealed a 12.0 X 11.3 cm inhomogeneous, well-enhancing soft tissue mass with small calcific and necrotic foci in the left half of abdomen (Figure 1). The left kidney was displaced downwards and malrotated with its long axis lying horizontally. FNAC was suggestive of ganglioneuroma. The 24-hour urinary Vanilmandelic acid (VMA) level was 68 micromoles (N < 35 micromoles/24 hours). On exploration a large, rounded, firm mass was present on the left side. Only the hilum and a part of the kidney were visible on the inferior aspect of the tumour. The plane of cleavage between the tumour and the kidney could not be established and the tumour was removed along with the kidney. Grossly, the tumour measured 16 X 14 cm, weighed 1 kg and on cut section had a greyish white surface. Histopathology revealed mature ganglion cells singly or in small nests along with spindle cells (Figure 2). Sections of the renal parenchyma showed no involvement except splitting of the capsule by the tumour tissue. The ureter and vein were unaffected but nerve tissue bundles were present around the outer coat of the renal artery. The tumour was reported as ganglioneuroma. DISCUSSION Ganglioneuromas represent the fully differentiated tumour of the sympathetic nervous system. These tumours may arise either by the spontaneous maturation of malignant neuroblastoma or may be diagnosed as primary ganglioneuroma. The exact incidence of ganglioneuromas is not known1 but they are quite rare compared with other benign neural tumours such as neurilemoma and neurofibroma.2 Usually, these tumours are regarded as adult tumours and the majority of the patients are 10 years and above;3 in contrast our patient was only four years old. Predominance in the female sex by 3:2 has been reported with an interesting observation that maturation of tumour cells takes place more readily in the females.2 They are found more frequently in the posterior mediastinum than in any other single location and in the abdomen they are widely distributed throughout the lumbar and pelvic retroperitoneal tissues, gastrointestinal tract and the mesentery. However, their occurrence in the adrenal is uncommon;1 only 15-20% of all reported ganglioneuromas arise in the adrenal gland.4 Usually, ganglioneuromas grow slowly and may attain large dimensions, becoming clinically evident because of the compression of adjacent structures. However, most of them remain asymptomatic and are diagnosed incidentally by imaging studies for unrelated reasons. Some abnormality in the catecholamine synthesis leading to the excretion of VMA and Homovanillic acid has been observed in about 39% of the patients;5 it rarely leads to hypertension but provides a very sensitive test for their detection. The 24 hour urinary VMA level was raised in our patient also. Sometimes chronic intractable diarrhoea may be the presenting symptom, especially in childhood, due to the presence of vasoactive intestinal peptide within the tumour.3 A variant of this syndrome characterized by hypokalemia and hypochlorhydria has also been described.2 Both these syndromes disappear after the removal of the tumour. Occasionally, ganglioneuromas are multiple and may be regarded as a variant of von Recklinghausen's disease when the skin is involved. Imaging studies show a well-circumscribed, homogenous mass with an interesting tendency to partially or completely surround blood vessels, without compromising the lumen in most cases. Grossly, ganglioneuromas are well-circumscribed encapsulated masses of firm consistency with a homogenous, solid greyish white cut surface. Histologically, they consist of bundles of longitudinally and transversely oriented Schwann cells with mature ganglion cells scattered throughout singly or in small nests. Although ganglioneuromas are benign tumours, rarely, an apparent metastatic focus of ganglioneuroma may be encountered within a lymph node adjacent to the main tumour mass or in a more distant site; it is assumed that these cases represent neuroblastoma in which the metastasis as well as the primary tumour matured;3 however, surgical excision effects cure in all the patients. The ganglioneuromas are benign tumours; adequate surgical excision effects cure in all the patients. Although ganglioneuromas occur rarely in small children, they should be considered in the differential diagnosis of adrenal masses. REFERENCES
© 2003 Indian Journal of Surgery. Also available online at http://www.indianjsurg.com The following images related to this document are available:Photo images[is03088f2.jpg] [is03088f1.jpg] |
| |||||||||

{kind=link}
{kind=link}