 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 65, No. 5, Sept-Oct, 2003, pp. 438-440 Case Report Lethal midline granuloma - epitheloid angiosarcoma face Leo Francis Tauro, Sathyamoorthy Aithala, Leo Theobald Menezes, Nandakishore B.*
Department of General Surgery and *Dermatology, Fr. Muller's Medical College
Hospital,Kankanady, Mangalore 575002. D.K., Karnataka.
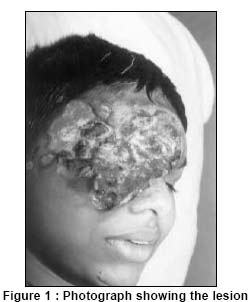
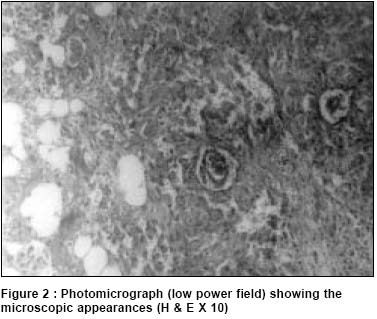
Paper Received: August 2000. Paper Accepted: January 2002. Source of Support: Nil. How to cite this article: Tauro LF, Aithala S, Menezes LT. Lethal midline granuloma - epitheloid angiosarcoma face. Indian J Surg 2003;65:438-40. Code Number: is03089 ABSTRACT Angiocentric immunoproliferative and locally destructive lesions involving the midface, nasal cavity, paranasal sinuses and / or the upper aerodigestive tract have been referred to in the past as lethal midline granuloma. This includes neoplastic, infective, vasculitic and idiopathic midline destructive disease. We report such a case of neoplastic origin which presented with necrotising lesion of the mid-face involving the right orbit and the nasal bridge. Histologically, it was proved to be angiosarcoma and was treated with chemotherapy. Key Words: Lethal midline granuloma, Angiosarcoma. INTRODUCTION Lethal midline granuloma (LMG) describes lesions of the mid-face which are characterised by progressive and often fatal ulceration and destruction of the upper airway involving the nose, the paranasal sinuses, the palate, orbit and the soft tissues of the face. Four entities are included under this term: idiopathic midline destructive disease (IMDD), polymorphic reticulosis, non-Hodgkin's lymphoma and Wegener's granulomatosis.1,2 We report a case of necrotising lesion of the mid-face involving the right orbit and the nasal bridge. CASE REPORT A 14-year-old boy presented with 1½ years history of painful ulcerative lesion over the face. The lesion started following a nail prick injury, as multiple papules at the lateral canthus of the right eye, which later ulcerated. The ulcer had been spreading since 9 months. General and systemic examination including that of the respiratory system revealed no abnormality. Local examination showed a destructive, ulcerative lesion involving the entire right orbital region, bridge of the nose and crossing the midline. The lesion had sloping edges, slough and unhealthy granulation at the floor, and was indurated as well as tender. The base was formed by underlying bone. The right eyeball was completely destroyed. There was no bleeding on touch and sero purulent discharge was present from the ulcer (Figure 1). Our clinical differential diagnosis was cancrum orbitalis and nasalis, LMG and actinomycosis face. Routine haematological and biochemical investigations were normal except an ESR of 65 mm/hr. Staphylococcus aureus and E. Coli were cultured from the wound. Skull X-ray showed orbital bone destruction. Chest x-ray was normal. CT scan showed extensive bone destruction involving the medial wall and floor of the orbit, the orbital fissure and sphenoid bone. There was a small extradural collection in the right frontal region and osteomyelitis of the right frontal bone. All these features pointed to an inflammatory pathology. Biopsy from the edge and base of the ulcer showed epitheloid angiosarcoma (Figure 2). Since the growth was extensive and inoperable, the patient was treated with chemo and radiotherapy. DISCUSSION Angiocentric immunoproliferative lesions involving the mid-face, nasal cavity, paranasal sinuses, and / or upper aerodigestive tract have been referred to in the past as LMG.3 When neoplastic, infective, vasculitic causes have been excluded, the diagnosis of IMDD is possible.4 Angiosarcoma of the skin is a rare malignant tumour which occurs in both sexes. Often, in elderly individuals it occurs either in a chronic lymphoedematous limb, e.g. in an arm after a radical mastectomy and radiotherapy for breast cancer or in the head and neck region in the scalp.5 Some of these lesions have been associated with foreign material introduced into the body either iatrogenically or accidentally.6 The tumour presents as red plaques and nodules which may be very extensive and which tend to ulcerate. Microscopically, the tumour consists of an anastomosing network of vascular channels, lined by atypical endothelial cells, dissecting through the dermal collagen. Areas of poorly differentiated solid spindle cell appearance may be present.5,6 The prognosis is very poor. These lesions often metastasise to the regional lymph node and distant sites, but death may occur before development of metastses in head and neck tumours as a result of extensive local destruction. REFERENCES
© 2003 Indian Journal of Surgery. Also available online at http://www.indianjsurg.com The following images related to this document are available:Photo images[is03089f1.jpg] [is03089f2.jpg] |
| |||||||||

{kind=link}
{kind=link}