 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
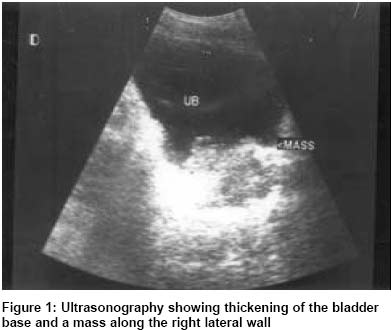
Indian Journal of Surgery, Vol. 65, No. 5, Sept-Oct, 2003, pp. 444-445 Case Report Cystitis cystica glandularis presenting as bladder tumour: A diagnostic dilemma M. S. Ansari, S. Dash, Daresh S. Doddamani, A. Seth Department of Urology, All India Institute of Medical Sciences, New Delhi
110029.
Paper Received: June 2002. Paper Accepted: September 2002. Source of Support: Nil. How to cite this article: Ansari MS, Dash S, Doddamani DS, Seth A. Cystitis cystica glandularis presenting as bladder tumour: A diagnostic dilemma. Indian J Surg 2003;65:444-5. Code Number: is03093 ABSTRACT A 25-year-old man presented with painless haematuria. Ultrasonography of the abdomen revealed thickening of the bladder base and a mass along the right posterolateral wall along with right hydroureteronephrosis. Transurethral resection of the mass (TUR) was done and histopathology revealed cystitis cystica glandularis. Key Words: Cystitis cystica glandularis, Bladder tumour. INTRODUCTION Cystitis cystica glandularis is a form of proliferative cystitis, which can be mistaken for bladder tumour clinically and radiologically. The condition is usually diagnosed after bladder biopsy for subtle mucosal changes or gross mucosal oedema. Cystoscopy may show a papillary lesion although often it is not grossly visible. An overt bladder mass is extremely rare. We present a case of cystitis cystica glandularis presenting with haematuria and bladder mass. CASE REPORT A 25-year-old man presented with painless haematuria for a period of 6 months. Routine laboratory investigations were normal. Urine AFB, PCR and cytology did not reveal any abnormality. X-Ray KUB region was normal. Ultrasonography abdomen revealed thickening of the bladder base and a mass along the right posterolateral wall along with right hydroureteronephrosis (Figure 1). Cystoscopic examination confirmed the findings of ultrasonography. The surface of the mass was nodular, partially cystic. Transurethral resection of the mass (TUR) was done and histopathology revealed cystitis cystica glandularis. DISCUSSION Cystitis cystica glandularis is a rare disease, caused by metaplasia of the vesical submucosa, probably related to a chronic irritative factor.1 Some investigators believe that this condition reflects mobilisation of the humoral immune defence response by various agents.2 In its minor form, it has the same clinical features as simple cystitis, but its major pseudoneoplastic form may be clinically mistaken for bladder tumour. Cystitis cystica glandularis is considered to be a premalignant disease of the urinary bladder as some reports document its progression to adenocarcinoma. It has also been reported to occur frequently in association with pelvic lipomatosis.3 Cystoscopic biopsy is mandatory, as the diagnosis is essentially histological. It appears histologically as submucosal nests of columnar epithelial cells surrounding a central liquefied region of columnar degeneration. In the absence of obvious lesion, treatment is usually medical, based on the eradication of the irritative factors. Surgery is required in case of complications of the disease like recurrent haematuria or features associated with bladder outlet obstruction secondary to the pseudoneoplastic growth. The surgical approach includes transurethral resection of the lesion (TUR) or laser ablation.4,5 The clinical course is unclear and requires long-term surveillance. REFERENCES
© 2003 Indian Journal of Surgery. Also available online at http://www.indianjsurg.com The following images related to this document are available:Photo images[is03093f1.jpg] |
| |||||||||

{kind=link}