 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 65, No. 5, Sept-Oct, 2003, pp. 445-446 Case Report Delayed presentation of a massive sub-capsular haematoma of the spleen Pinaki Mukhopadhyay Department of Surgery, Assembly of God Hospital and Research Center, 125/1,
Park Street, Calcutta 700017.
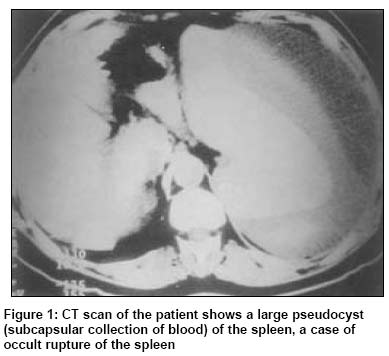
Paper Received: June 2001. Paper Accepted: August 2002. Source of Support: Nil. How to cite this article: Mukhopadhyay P. Delayed presentation of a massive sub-capsular haematoma of the spleen. Indian J Surg 2003;65:445-6. Code Number: is03094 ABSTRACT The spleen remains one of the most commonly injured organ in patients sustaining blunt abdominal trauma.1 Splenic rupture may be acute (over 90%), delayed (approx.10%) or occult.2 The occult rupture of the spleen, an extremely rare condition, refers to traumatic pseudocyst formation around the spleen, when the primary injury of the organ was not diagnosed and was overlooked. Later on, the patient presents with abdominal lump, pain or heaviness in the left upper abdomen. These patients are usually anaemic but characteristic acute features of splenic rupture are absent. Splenectomy cures the condition. We report one such case who presented with a large splenic haematoma. Key Words: Spleen, Injury, Occult rupture, Pseudocyst, Abdominal trauma. INTRODUCTION In blunt abdominal trauma, the spleen is one of the most commonly injured organ. The splenic rupture may be acute, delayed or occult in nature.2 Acute rupture, characterised by intraperitonial bleeding and features of shock, occurs in more than 90% of cases. Delayed rupture is seen in less than 10% of cases. These patients present after an interval of days or weeks (latent period of Baudet)3 from the original injury. The entity of delayed splenic rupture is often challenged.4 We report a patient who presented with a large splenic haematoma several seeks after injury. CASE REPORT A 57-year-old male patient was admitted with a progressively painful lump in the left upper abdomen of 3 weeks duration. He also complained of weakness for the same duration. Some 3 weeks ago he had been treated following a fall down a manhole. A chest x-ray (PAView) taken at that time had shown no abnormality and he was sent home. He was apparently better but never free of symptoms. Thereafter, he noticed a progressively painful lump in the upper abdomen on the left side. He also developed weakness which was progressive in nature. Hematological and biochemical investigations were normal except a haemoglobin of 5 .6 gm%. A left oblique chest x-ray showed a fracture of the left seventh rib and ultrasonography identifies splenic injury with a large encapsulated haematoma; there was no free fluid in the peritoneal cavity. A computerised tomography (CT) (Figure 1) showed a large subcapsular haematoma and laceration of the lateral surface of the spleen. The patient was diagnosed to have suffered an occult rupture of the spleen. At splenectomy a large encapsulated haematoma over the lateral surface of the spleen was found. The postoperative period was uneventful and the patient was discharged on the eighth postoperative day. DISCUSSION As spleen is the most commonly injured organ in blunt abdominal trauma1, all cases with a history of trauma in the region of the lower chest or upper abdomen on the left side, should be suspected for injury to the spleen and thoroughly investigated. A detailed history and clinical examination are mandatory. Ultrasonography and CT scan should be done at the slightest suspicion of intra-abdominal injury. If a fracture of the ribs (which forms the splenic bed) is present, it raises further doubts about splenic injury though its presence or absence neither confirms nor excludes rupture of the spleen. A left oblique view of the chest is necessary to detect such a fracture as posteroanterior view may not always reveal the injury. Occult rupture is an extremely rare condition, when there is formation of traumatic pseudocyst (blood) around the spleen.2 The splenic capsule remains intact. Nevertheless, this condition may be accompanied by severe loss of blood.6 The original injury is usually undiagnosed or overlooked. Victims of occult rupture of the spleen present late with features of a lump in the left upper abdomen, anaemia and pain. The typical features of splenic rupture are absent and the presentation takes more of an insidious course. The diagnosis is easily made with USG and CT scan of abdomen. Splenectomy cures the condition. However, awareness and thorough clinical examination, supplemented by investigation when required, are necessary to prevent misdiagnosis of splenic injury at the first instance. REFERENCES
© 2003 Indian Journal of Surgery. Also available online at http://www.indianjsurg.com The following images related to this document are available:Photo images[is03094f1.jpg] |
| |||||||||

{kind=link}