 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
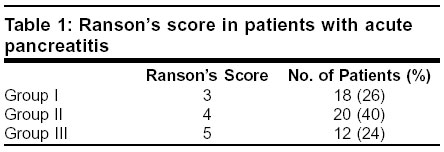
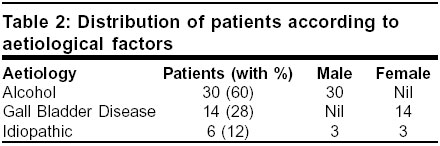
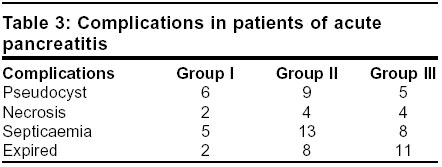
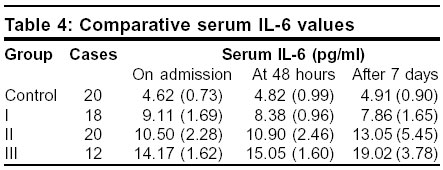
Indian Journal of Surgery, Vol. 65, No. 6, November-December, 2003, pp. 480-482 Evaluation of the prognostic role of inflammatory markers: Tumor necrosis factor (TNF-α) and interleukin-6 (IL-6) - in patients with acute pancreatitis Kuldip Singh, A. P. Narang,* R. P. Singh, S. C. Goyal Departments of Surgery and *Biochemistry, Dayanand Medical College & Hospital, Ludhiana - 141001, India. Paper Received: March 2003. Paper Accepted: July 2003. Source of Support: Nil. How to cite this article: Singh K, Narang AP, Singh RP, Goyal SC. Evaluation of the prognostic role of inflammatory markers: Tumor Necrosis Factor (TNF-α) and Interleukin-6 (IL-6) - in patients with acute pancreatitis. Indian J Surg 2003;65:480-2. Code Number: is03103 ABSTRACT Acute pancreatitis is one of the poorly understood common acute digestive tract disorders. It is not just difficult to diagnose, even the severity of the disease is often underestimated. Early in the course of pancreatitis, pro-inflammatory agents can release more cytokines like TNF-α and IL-6 into the pancreatic tissue and serum, thereby amplifying the local and systemic inflammatory response. In the present study, 50 patients diagnosed on the basis of routine investigations, imaging techniques and history as having acute non-traumatic pancreatitis and falling between Ranson's criteria 2 and 6, were studied. They were divided into Groups I, II and III with Ranson's criteria of 3, 4 and 5 respectively. In addition to routine investigations, serum Interleukin-6 (IL-6) and Tumour Necrosis Factor (TNF-α) values were measured on the day of admission, after 48 hours and on the seventh day. A control group of 20 patients with pain abdomen of non-pancreatic origin were investigated, studied and closely followed up simultaneously. Alcohol was found to be the major positive factor (60%), with gallstones found in 28%. Both IL-6 and TNF-α were significantly increased in patients with acute pancreatitis as compared to patients of non-pancreatic pain abdomen. The levels were significantly higher in Group III when compared with Groups I and II. Although values of IL-6 and TNF-α are increased significantly, they do not play any significant role in predicting the outcome of acute pancreatitis. Since our study was on a small scale and as our patients reached after wasting interventional time, a prospective study on a much larger scale, without any disadvantage of the time factor would be a welcome effort in this field of vast possibilities. Key words: Acute pancreatitis, IL-6, TNF-α. INTRODUCTION Acute pancreatitis has varied clinical manifestations, is difficult to diagnose, has an unpredictable course, and is even more difficult to prognosticate. It is a protean disease ranging from mild discomfort to catastrophic results, with high morbidity and mortality. It is characterized by abdominal pain and elevation in the serum levels of amylase and lipase. A key feature of acute pancreatitis is the elaboration of an inflammatory reaction which results in oedema of the pancreas as extensive local and systemic effects. On the basis of data of patients in USA, Asia and Western Europe, gallstones account for approximately 45% cases of acute pancreatitis, alcohol for 35%, other causes for 10%, and the remaining 10% are idiopathic.1 Serum lipase assay has more sensitivity and specificity in the diagnosis. Imaging techniques remain a sensitive method of evaluating the biliary tract in acute pancreatitis. Ranson's criteria have been largely accepted to which others have suggested modifications.2,3 The Acute Physiologic Assessment and Chronic Health Evaluation (APACHE-II) is another study of prognostic indications.4 Early in the course of pancreatitis, serum and intrapancreatitic levels of a number of cytokines are elevated.5,6 Pro-inflammatory agents attract neutrophils and macrophages, which can release more cytokines, such as TNF-α, IL-1, IL-6, and nitric oxide into the pancreatic tissue and serum, thereby amplifying the local and systemic inflammatory response.7,8 IL-6 has been shown as a multifactorial cytokine secreted by normal cells, cell linen and tumour cells, and it is an important mediator of the inflammatory response, not only in acute pancreatitis, but in all other acute inflammatory responses as well.9,10 Besides IL-6, the other significant mediator which could throw light on the prognosis of acute pancreatitis is TNF-α. It is a cytokine elaborated by macrophages. It is the primary cytokine mediating various inflammatory responses. Keeping in view these points, the present study was planned to establish any correlation between serum values of immunoreactive IL-6 and TNF-α, and the positive diagnosis of acute pancreatitis in patients presenting to the hospital with acute pain abdomen. MATERIAL AND METHODS The present study was carried out on 50 patients diagnosed as suffering from non-traumatic acute pancreatitis, admitted to the Dayanand Medical College and Hospital, Ludhiana. The diagnosis of acute pancreatitis was based on: clinical picture suggestive of acute pancreatitis, increase in levels of serum amylase and lipase to more than 2.5 times the normal values, and USG/CT scan of abdomen. Ranson's scoring was done at admission and repeated at 48 hours. Patients having scores less than 6 but more than 2 were included in the study and were further divided into three groups (Table 1). Out of 50 patients, 32 were males and 18 were females. They were in the age group of 20-78 years. Acute pancreatitis was labelled as being of alcoholic origin in cases giving history of prolonged alcohol abuse for months to years or those with history of heavy alcohol intake within four days of the attack of acute pain abdomen. The standard imaging technique of ultrasonography was used to label a case as that of gall bladder disease, especially of gallstone origin. If both the above histories were negative and there was no history of operative or diagnostic interventional trauma, the case was labelled as idiopathic (Table 2). A second group of 20 patients with pain abdomen of non-pancreatic origin, matched in terms of age and sex, were studied as the control group. In addition to routine tests (serum sugar, urea, creatinine, electrolytes, bilirubin, SGOT, SGPT, ALP, LDH, amylase, lipase), IL-6 and TNF-α were estimated at the time of admission, after 48 hours and after 7 days. Both IL-6 and TNF-α were determined by Immunotech kits, an enzymatic immunoassay method. The minimum detectable concentration for IL-6 and TNF-α was 1 pg/ml. The data collected was subjected to the Chi-sqaure test to compare among different groups. RESULTS In spite of intensive initial treatment, most patients developed complications which led to an increase in morbidity and mortality. Septicaemia and pseudocyst formation were the major complications seen. Out of 50, 20 patients developed pseudocyst, 10 developed pancreatic necrosis, 26 septicaemia and 21 patients expired (Table 3). Treatment in the form of prophylactic antibiotics was given to all patients. Surgical intervention in the form of necrosectomy was done in 6 patients, laproscopic cholecystectomy in 2 patients, percutaneous drainage in 9 patients, and pleural tap in 1 patient. No surgical intervention was done in 32 patients. In the control group of 20 patients, serum IL-6 levels were between 3.0 and 6.9 pg/ml. These levels were significantly higher in all the three groups of patients with acute pancreatitis, when estimated at three different intervals: at admission, at 48 hours, and at 7 days (P<0.001). IL-6 was significantly increased in Group III as compared to Groups I and II (Table 4). The TNF-α in the controls ranged between 3.2 to 6.2 pg/ml. It was significantly higher in all the three groups of patients of acute pancreatitis when estimated at different intervals (P<0.001). Also, it was significantly higher in Group III when compared to Groups I and II (Table 5). DISCUSSION In spite of various experimental and interventional studies in acute pancreatitis, an accurate predictor of the outcome of acute pancreatitis still eludes us. The present study is another step in this direction. The ideal prognostic indicator should be accurate, simple, non-invasive, detectable early and should firmly predict the course of the disease. IL-6 is a member of the inflammatory cytokine family, and is well characterized as the primary inducer of the acute phase protein response during all types of insults, in direct correlation with their severity.11 Similarly, the role of TNF-α has been examined as the initiator of local and systemic damage occurring during acute pancreatitis.2 Acute pancreatitis remains a common and potentially fatal disease in which some patients develop extensive pancreatic inflammation and necrosis, a systemic inflammatory response and multiple organ failure.12 It has been reported that markers of inflammation in the sera of patients with acute pancreatitis are highest in those who subsequently develop organ failure. Both IL-6 and TNF-α were on the higher side in those patients who developed fatal complications. The role of IL-6 and TNF-α as predictors of the outcome of acute pancreatitis appears to be promising. That day is not far when these inflammatory mediators will find due importance as prognostic indicators of significance. The earlier the patient is investigated for serum values of IL-6 and TNF-α, the more conclusive are the results as far as their predictive values are concerned. In the present study, the time factor appeared to be the major hurdle in the way of drawing any firm conclusion. Most patients reached us after a delay of some days, and these were the days when any significant investigation might have resulted. In the near future these inflammatory mediators will find due importance as prognostic indicators of significance. REFERENCES 1. Gorelick, FS. Acute pancreatitis. In: Yamada T, editor. Textbook of Gastroenterology. 2nd edn. Philadelphia: IB Lippinocott; 1994. pp. 2064-90. 2. Berry AR, Taylor TV. Diagnostic tests and prognostic indication in acute pancreatitis. J Royal Coll Surg Edin 1982;27:345-52. 3. Blamey SL, Imrie CW, O'Neil J. Gilmour WH, Carter DC. Prognostic factors in acute pain. Gut 1984;25:1340-6. 4. Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II. A severity of disease classification system. Crit Care Med 1985;13:818-29. 5. Norman J. The role of cytokines in the pathogenesis of acute pancreatitis. Ann J Surg 1998;175:76-82. 6. Grady T, Liang P, Ernst SA, Logsdon CD. Chemokine gene expression in rat pancreatic acinar cells in an early event associated with acute pancreatitis. Gastroenterology 1997;113:1966-75. 7. Terrenhoir O, Nordback I, Isolauri. Influence of pancreatic resection on systemic complication in ANP. Br J Surg 1988;75:793-5. 8. Leser HG, Gross V, Scheibenbogen C, Heinisch A, SalmR, Lausen M, et al. Evaluation of serum IL-6 concentration precedes acute phase response and reflects severity in acute pancreatitis. Gastroenterology 1991;101:782-5. 9. Shalaby MR, Waage A, Aasden C, Espevik T. Endotoxin, TNF-α and IL-1 induce IL-6 production in vivo. Clin Immunol Immunopathol 1989;53:488-98. 10. Viedma JA, Pirez-Mateo M, Agullo J, Dominguez JE, Carballo F. Inflammatory response in the early prediction of severity in human acute pancreatitis. Gut 1994;35:822-7. 11. Kishimoto T, Akira S, Narazaki M, Taga T. Interleukin-6 family of cytokines. Blood 1995;86:1243-8. 12. de Beaux AC, Goldie AS, Ross JA, Carter DC, Feron KC. Serum concentrations of inflammatory mediators related to organ failure in patients with acute pancreatitis. Br J Surg 1996;83:349-52. © 2003 Indian Journal of Surgery. Also available online at http://www.indianjsurg.com
The following images related to this document are available:Photo images[is03103t3.jpg] [is03103t5.jpg] [is03103t2.jpg] [is03103t4.jpg] [is03103t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}