 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 65, No. 6, November-December, 2003, pp. 488-491 Prolene hernia system in the tension-free repair of primary inguinal hernias Vinod A. Chandiramani, Avinash N. Katara, Shefali M. Pandya, Nita S. Nair Department of General Surgery, P. D. Hinduja National Hospital & Medical Research Centre, Veer Savarkar Marg, Mahim, Mumbai - 400016, India.
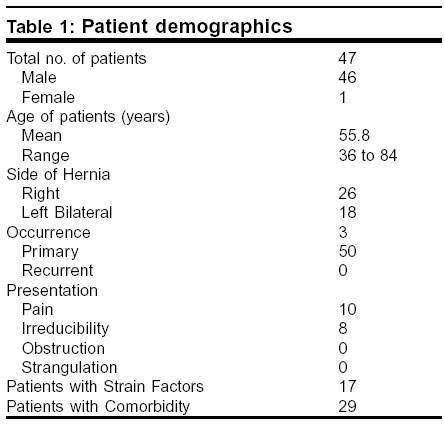
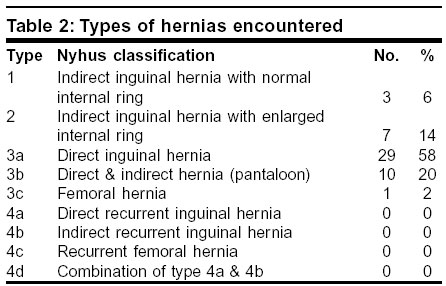
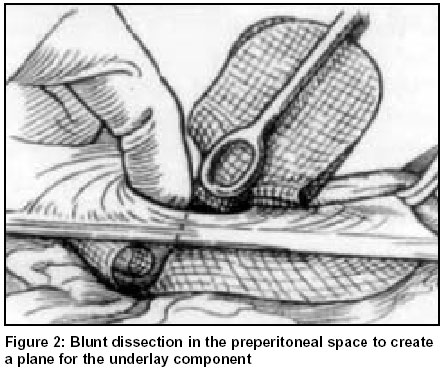
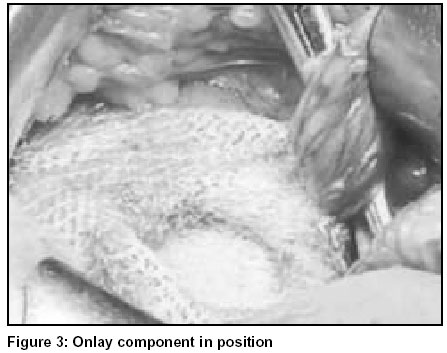
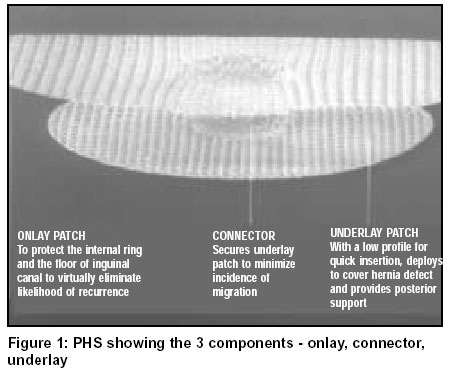
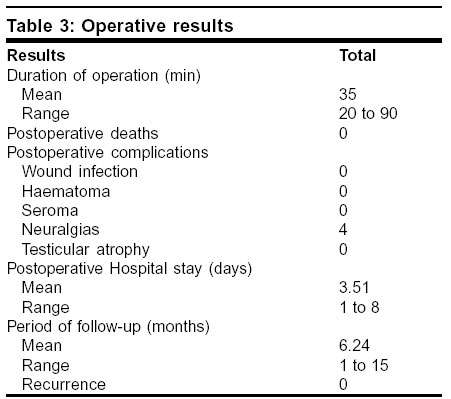
Paper Received: June 2003. Paper Accepted: August 2003. Source of Support: Nil. How to cite this article: Chandiramani VA, Katara AN, Pandya SM, Nair NS. Prolene hernia system in the tension-free repair of primary inguinal hernias. Indian J Surg 2003;65:488-91. Code Number: is03105 ABSTRACT Objective: The aim of this study was to determine the feasibility of using the Prolene® (polypropylene) Hernia System for open tension-free repair on inguinal hernias, and study the results in terms of operation time, patient comfort, hospital stay, return to normal activity and postoperative complications. Key Words: Prolene hernia system, Tension-free inguinal hernioplasty. INTRODUCTION Tension-free mesh repairs for adult inguinal hernias were originally popularized by Lichtenstein et al,1 in 1989 and have been gaining popularity ever since. Tension-free mesh repairs through the anterior approach are simple to perform and give excellent results with less postoperative pain and discomfort, a more rapid return to regular activities and lower recurrence rates.2 The Prolene® (polypropylene) Hernia System (PHS) [registered product, Ethicon, Inc.] is a novel concept developed for tension-free repairs of inguinal hernias. We report our initial experience with the PHS used in 50 cases over a period of 15 months. MATERIAL AND METHODS From February 2002 through April 2003, we performed open tension-free repair of inguinal hernia using the The ages of these patients ranged from 36 to 84 years, with a mean age of 55.8 years. There were 26 right and 18 left hernias. 3 patients had bilateral hernias, which were repaired simultaneously. A total of 50 hernias were observed in 47 patients (Table 1). We classified all hernias according to the Nyhus classification, and the percentage of each variety is shown (Table 2). There were 50 primary and no recurrent hernias in our series. Ten patients had pain as a presenting symptom. Eight patients gave a history of irreducibility. None of our patients gave a history suggestive of intestinal obstruction or strangulation in the past. Seventeen patients had a strain factor prior to surgery. The strain factors included cough (4), constipation (5), bladder outlet obstruction (4) or lifting heavy weights (4). Twenty-nine patients had comorbid conditions like hypertension (12), ischaemic heart disease (2), bronchial asthma (4), diabetes mellitus (6), cerebrovascular disease (2), cirrhosis (1), heartblock (1) and tertiary syphilis (1). SURGICAL TECHNIQUE A majority of our cases (35) were performed under local anaesthesia using an inguinal field block with 20 ml of 2% lignocaine with adrenaline. In 9 patients, general anaesthesia was used because of either large irreducible or bilateral hernias or when other procedures were carried out simultaneously. Three patients, who were found unfit for general anaesthesia, were given spinal anaesthesia for similar indications. An oblique 4-5 cm skin incision was made in the inguinal region, and the inguinal canal was opened in layers. The cord structures were looped up in the region of the pubic tubercle and held. The cremaster was incised and the cord structures and hernial sac were dissected from it by blunt and sharp dissection. The hernial sac was then delineated and dissected free from the cord structures. Indirect sacs were inverted and reduced into the peritoneal cavity, or alternatively twisted, transfixed and excised. The transversalis fascia covering the posterior wall of the inguinal canal was cut open for a length of 2 cm. With blunt dissection using a finger and gauze, the preperitoneal space of Bogros was dissected out to create a plane for the underlay part of the mesh. The underlay patch was spread out in the preperitoneal space created (Figure 2), and the defect in the transversalis fascia was narrowed with one or two interrupted sutures of 2-0 polypropylene. In patients with a lax internal ring, the preperitoneal plane was created by passing a finger or a piece of gauze through the internal ring itself. The onlay mesh was then spread out over the posterior wall of the inguinal canal (Figure 3). This was fixed using 3-4 interrupted sutures of 2-0 polypropylene. Haemostasis was achieved and the inguinal canal closed in layers. If a pantaloon hernia was encountered, we ligated and cut the inferior epigastric vessels, thus converting the two areas into one large defect. This was then treated in similar way, by opening the transversalis fascia and deploying a PHS. A femoral hernia was encountered in one of our patients. The hernia was reduced through the inguinal approach, and the PHS was deployed, which effectively covered the hernial defect, as well as the potential inguinal hernial sites. We used prophylactic antibiotics for all our patients. Patients were given 3 doses of intravenous cefuroxime (1.5 gm, 12 hourly), followed by oral cefuroxime (500 mg, 12 hourly) for 5 days. Our patients received analgesics (50 mg diclofenac in 27 cases, 50 mg tramadol in 20 cases) 8 hourly for the first 2 days and as required thereafter. Discharge was scheduled according to the decision of the patient. RESULTS 47 patients had a tension-free hernioplasty using the PHS (Table 3). The duration of surgery averaged 35 min (range 20-90 min). There were no postoperative deaths. Four patients experienced neuralgia in the inguinal region. This was self-limiting and resolved spontaneously in about a week. There were no wound infections, no haematomas and no seromas. The average duration of postoperative hospital stay was 3.5 days (range 1-8 days). We have a follow-up period ranging from 1 month to 15 months, with an average of 6.24 months. We have had no recurrence so far. Our follow-up period is short, compared to studies using other methods of hernia repair. Long-term results are awaited. DISCUSSION Tension-free mesh repairs for adult inguinal hernias was originally popularized by Lichtenstein et al1 in 1989, although Liechtenstein himself credits Newman with the original description of this repair. It is widely accepted worldwide and is the most commonly performed tension-free repair today. The PHS has been developed for the tension-free repair of inguinal hernias. It provides 3 components of the most popular mesh devices in use today for open hernia repairs, in a single, easily used device. The 3 components include: 1. An underlay mesh similar to that used in Gilbert's sutureless repair3 The PHS is constructed of high-porosity polypropylene for optimum tissue ingrowth. It can be used to repair all types of inguinal hernias, including femoral hernias. The PHS has many theoretical advantages over the other conventional forms of repair. It provides a larger allowable surface for effective tissue ingrowth and fibrosis. The underlay patch lies in the preperitoneal space and provides a double-layered reconstruction of the transversalis fascia. The PHS protects both the femoral and inguinal regions from recurrence. The underlay component secures the myopectineal orifice and the onlay component secures the posterior wall of the inguinal canal. Placement of the underlay component in the preperitoneal plane has theoretical advantages. It employs Pascal's principle of hydrostatic pressure to allow the intra-abdominal pressure to keep the mesh secure in place. It has all the advantages of a secure posterior repair from a simple anterior approach. It is a versatile prosthesis that can be used for other abdominal wall hernia repairs. Most of our patients were operated under local anaesthesia. Apart from averting all the complications of general anaesthesia, it allowed patients to cough and strain during the procedure to identify additional hernias. We were able to test competency of the repair on table, and patients were able to walk and void immediately after surgery. The average hospitalization for our patients was 3.5 days. Most of our patients who underwent surgery under local anaesthesia became ambulatory very soon after surgery. Most of them were fit for discharge 1 or 2 days after surgery, and returned to work in 7-10 days. Some patients stayed longer for medical reasons. The average hospital stay of our patients also increased because 4 patients underwent other procedures simultaneously (2 cystoscopies with internal urethrotomies, 1 orchidectomy, 1 TURP with cystolithotrity). In addition, on account of logistical reasons such as outstation residence and co-morbidity factors, a few patients wished to stay until suture removal. Few of our patients were well motivated and undertaken as day care patients. Early reports of this device are encouraging. Operating time is shorter and there is quicker recovery.5-7 The PHS theoretically provides all the advantages of a tension-free repair, including less patient discomfort, rapid return to normal activity and lower recurrence rates. These benefits have been observed in the limited time period of case studies so far. In addition, it is easy to use, requires fewer sutures for fixation and is more comfortable for the patient in the postoperative period, in our experience. It provides a stable anterior repair with the added benefits of a posterior repair and plug repair. The higher cost of the PHS as compared to the conventional polypropylene mesh makes its widespread use difficult. There are patients undergoing conventional tension-free hernioplasties who develop recurrence. Univariate analyses for prognostic variables of recurrence8 have pointed out several risk factors for recurrence, viz. increased age, female sex, preoperative pain, operation time, type of hernia (Nyhus 2,3,4), conversion to another procedure, type of operation (e.g. tension-free vs. Bassini's repair or other tension repairs), presence of haematoma or wound infection. These `high-risk' group of patients may be a good target to analyze the role of the PHS as a superior primary repair. Even recurrences should be tackled with the PHS where an area on the posterior wall with relatively fewer adhesions, usually on the medial half, can be used as an approach to create the preperitoneal plane. Randomized double-blind prospective trials are needed to actually ascertain the potential benefits of the PHS over the conventional polypropylene mesh. CONCLUSION The Prolene Hernia System is a novel approach in the management of inguinal hernias, with encouraging initial results. The cost factor may be a major drawback, especially in developing countries. Its long-term efficacy needs to be studied with larger, prospective double-blind randomized trials, with longer follow-up. REFERENCES 1. Lichtenstein IL, Shulman AG, Amid PK, Montllor MM. The tension-free hernioplasty. Am J Surg 1989;157:188-93. 2. Kark AE, Kurzer M, Waters KJ. Tension-free mesh repair: review of 1098 cases using local anaesthesia in a day unit. Lancet 1999;354:175-6. 3. Gilbert AI, Graham MF. Improved sutureless technique _ advice to experts. Problems in General Surgery 1995;12:117-9. 4. Rutkow IM, Robbins AW. Tension-free inguinal hernioplasty: a preliminary report on the mesh plug technique. Surgery 1993;114:3-8. 5. Yamamato S, Maeda T, Uchida Y, et al. Open tension-free mesh repair for adult inguinal hernia: eight years experience in a community hospital. Asian J Surg 2002;25:121-5. 6. Kingsnorth AN, Wright D, Porter CS, Robertson G. Prolene hernia system compared with Lichtenstein patch: a randomized double blind study of short-term and medium-term outcomes in primary inguinal hernia repair. Hernia 2002;6:113-9. 7. Murphy JW. Use of the prolene hernia system for inguinal hernia repair: retrospective, comparative time analysis versus other inguinal hernia repair systems. Am Surg 2001;67:919-23 8. Liem MSL, van Duyn EB, van der Graaf Y, van Vroonhoven JM. Recurrences after conventional anterior and laparoscopic inguinal hernia repair: a randomised comparison. Ann Surg 2003;237:138-141. © 2003 Indian Journal of Surgery. Also available online at http://www.indianjsurg.com The following images related to this document are available:Photo images[is03105t3.jpg] [is03105f2.jpg] [is03105f3.jpg] [is03105t2.jpg] [is03105t1.jpg] [is03105f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}