 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 65, No. 6, November-December, 2003, pp. 492-495 Precholecystectomy ERCP in follow up cases of gallstone pancreatitis. Is it necessary? Subrat Raul, Sudhir Joseph, Hansa Shahi, Ashish Bhagat, Neerav Goyal Departments of Surgery, Gastroenterology & Radiology, St Stephen's Hospital, Delhi, India.
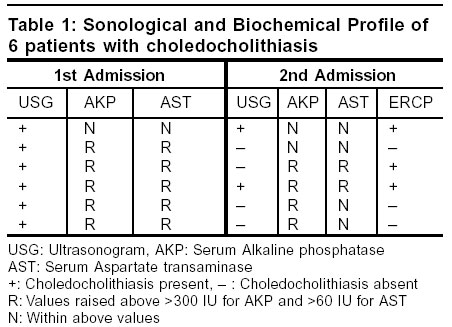
Paper Received: June 2003. Paper Accepted: September 2003. Source of Support: Nil. How to cite this article: Raul S, Joseph S, Shahi H, Bhagat A, Goyal N. Precholecystectomy ERCP in follow up cases of gallstone pancreatitis. Is it necessary? Indian J Surg 2003;65:492-5. Code Number: is03106 ABSTRACT Background/Objective: The need for a routine ERCP prior to cholecystectomy in all follow up cases of gallstone pancreatitis; the incidence of choledocholithiasis in these cases and to define radiological and biochemical criteria that would necessitate a precholecystectomy ERCP. Key words: Gallstone pancreatitis, ERCP, Cholecystectomy, CBD. INTRODUCTION Acute pancreatitis is a common disease with considerable morbidity and mortality.1-3 The disease has a varied aetiology; gallstone disease and alcohol predominating amongst identifiable causes. In the UK the reported incidence of gallstone pancreatitis has been variable. Studies report that biliary stone disease accounts for 30% to 50% of cases of acute pancreatitis.2-6 Recognized management of acute gallstone pancreatitis is to ensure that any choledocholithiasis is diagnosed and cleared with definitive eradication of gallstones by cholecystectomy. ERCP can be used to diagnose and clear choledocholithiasis but eradication of gallstones is by cholecystectomy (laparoscopic or open).7 At our centre we follow the traditional approach of allowing the acute attack of pancreatitis to settle in severe cases, discharge the patient and arrange readmission for cholecystectomy, 4-6 weeks later. The cholecystectomy was always preceded by ERCP. This approach of deferred surgery though, has its drawbacks as data show that as many as 50% of patients will experience further attacks of pancreatitis during the waiting period.8-10 However all the patients in this study group had documented severe acute pancreatitis based on Ranson's scoring system and radiological evaluation by CT scan, correlated with Balthazer classification of severity which in any case precluded early surgery. We evaluated the need for ERCP prior to cholecystectomy in all these cases. There are reports favouring the policy of early or even emergency ERCP, endoscopic clearance of CBD followed by surgery within 24-48 hours in severe cases. The reasons for following the traditional approach of deferred surgery in our institution have been; 1) most of these sick patients had single or multiple organ failure and it was thought not to intervene during this critical phase, 2) joint decision of our gastroenterologists and surgeons not to cannulate the CBD i.e. to perform an ERCP in the presence of ongoing inflammation except in cases where absolutely indicated, 3) our earlier experience of a high rate of conversion of laparoscopic to open cholecystectomy when early surgery was performed in these cases, 4) a low rate of less than 4% of recurrent pancreatitis during the waiting period for surgery and 5) reluctance of most patients to undergo surgery during the same admission. It is accepted practice that the optimal management of gallstone pancreatitis and CBD stones depends on the skills and resources available as well as patient preference.11 MATERIAL AND METHODS 42 patients of gallstone pancreatitis were managed in the period January - December 2001.The initial attack of acute pancreatitis was managed conservatively. During this period all biochemical parameters and radiological investigations relevant for the management of acute pancreatitis were performed. The severity of pancreatitis was based on the Ranson's scoring system. All these patients were advised to undergo cholecystectomy within 3-4 weeks following their acute attack. However only 36 patients turned up for definitive surgery and these form our study group. There were 10 males and 26 females with a median age of 34 years (range 17yrs-72yrs). During this admission for surgery, all these patients had an ultrasound of the abdomen and liver function tests. These were compared with the findings and values during their previous admission. All the above patients had ERCP prior to their cholecystectomy. RESULTS Ultrasound had detected gallstones in all the 36 cases during the phase of acute pancreatitis. In addition 6 cases had concomitant choledocholithiasis (Table 1). Derangements in the liver function tests (specifically AST and AKP) occurred in 20 cases. These included the 6 cases that had choledocholithiasis. All these 36 patients during their attack of acute pancreatitis had a Ranson's score of 3 or more at 48 hours after admission. Ultrasound however detected choledocholithiasis in only 2 cases during the second admission. The liver function tests were significantly deranged in 2 cases. ERCP detected stones in CBD in 3 cases which were cleared during the same time.34 cases underwent laparoscopic cholecystectomy and 2 had open cholecystectomy due to technical problems. Biliary tract pathology was not detected in any of the cases that did not show choledocholithiasis on ultrasonogram during the first admission. Follow up of more than 1 year in all these cases has been uneventful. DISCUSSION The first description of the association between gallstones and acute pancreatitis is variously attributed to Bernard (quoted by Kirchner et al) or Prince who reported impaction of a gallstone in a common channel just distal to the entry of the pancreatic duct.12,13 In 1901, Opie also described impaction of a stone in the lower common bile duct in a patient with fatal acute pancreatitis.14 Since then the role of gallstones as an etiological factor has been recognized increasingly, although the mechanism responsible remains controversial. Gallstones causing biliary pancreatitis produce only transient obstruction after which they pass spontaneously into the duodenum. Early trends in the serum pancreatic enzymes and liver function tests in patients with gallstone pancreatitis can predict persistent CBD stones and complications of pancreatitis.15,16 This subset of patients with persistent enzyme elevation would then benefit most from further biliary imaging and managed accordingly. Numerous efforts have been undertaken to define predictive criteria for common duct stones, but only a few provide practical guidelines for the prediction of stones.17-20 Even with the application of a predictive scoring system, only 42% of patients undergoing ERCP proved to have CBD stones. Age, the observation of bile duct dilatation or stones on ultrasonography, cholangitis and raised liver function tests are described as predictive criteria for CBD stones.20 In today's laparoscopic era, various trials have been performed to assess indicators for predicting choledocholithiasis before laparoscopic cholecystectomy. In a study by Alam21 where he grouped patients according to six indicators, 1) biliary pancreatitis, 2) jaundice, clinically and biochemically, 3) dilated bile duct on ultrasonography, 4) documented stones in CBD on sonography, 5) deranged liver functions in the absence of jaundice and 6) dilated bile duct on sonography with deranged liver functions, the best predictive values were in the group where ultrasound detected biliary duct stones followed by ultrasonographically detected dilatation of bile duct with deranged liver function tests. Deranged liver function tests alone was the least sensitive indicator. The use of an optimal model, by combining the predictive factors such as age, clinical jaundice, elevated alkaline phosphatase (ALP) dilated CBD or presence of stones in biliary tree on sonography will improve the sensitivity and patient selection for preoperative ERCP.22,23 Gallstone pancreatitis is a clear indication for a definitive biliary tract procedure intended to reduce the risk of recurrent attacks of pancreatitis. In the past definitive biliary tract surgery (open cholecystectomy plus cholangiography with or without common duct exploration) for gallstone pancreatitis was often delayed for upto 8 weeks after an episode of acute pancreatitis.16 This approach has however lost favour because of recurrent attacks of pancreatitis.8-10 Early surgery was deferred in our cases on account of the severity of acute pancreatitis based on the Ransons scoring system. The other reasons for following the traditional approach of delayed surgery which have been mentioned earlier are hereby reiterated. 1) most of these sick patients had single or multiple organ failure and it was thought not to intervene during this phase, 2) joint decision of our gastroenterologists and surgeons not to cannulate the CBD i.e to perform an ERCP in the presence of ongoing inflammation except in cases where absolutely indicated, 3) our earlier experience of a high rate of conversion of laparoscopic to open cholecystectomy when early surgery was performed in these cases, 4) a low rate of less than 4% of recurrent pancreatitis during the waiting period for surgery and 5) reluctance of most patients to undergo surgery during the same admission. In the present day of laparoscopic cholecystectomy, preoperative ERCP or intraoperative cholangiography is used to clear the biliary tree when a high index of suspicion for retained common bile stone exists.16 Cholecystectomy is still regarded as the definitive treatment of gallstone pancreatitis once the acute attack of pancreatitis settles.8,24 Controversy only exists regarding the timing of cholecystectomy. We evaluated the need for ERCP in all these cases prior to cholecystectomy. The indications of ERCP for evaluation of the common bile duct are well documented.25 It also has a valuable role when the cause of acute pancreatitis remains obscure. However from a purely diagnostic point of view MRCP today is considered a better alternative.26 Goodman reported 99 patients who were discharged following an attack of idiopathic acute pancreatitis.27 In spite of a normal ultrasonogram 7 out of 33 patients who underwent ERCP had biliary tract stones. In Hong Kong Lee et al have strongly recommended ERCP within 2 weeks of recovery from acute gallstone pancreatitis as a means of detecting biliary tract pathology.28 Tate et al carried out laparoscopic cholecystectomy at an interval of 3-24 days (Median & days) after admission in 24 patients with gallstone pancreatitis in whom clinical improvement had occurred. Preoperative ERCP was used routinely in this study and choledocholithiasis in 7 patients was dealt with endoscopically.29 The routine use of preoperative ERCP in every case was questionable. We addressed this particular issue in our study. Several studies have already addressed the issue of preoperative ERCP in gallstone pancreatitis. It is presently agreed that preoperative ERCP is not indicated for patients with mild gallstone pancreatitis. Alam21 recovered stones from CBD on ERCP in 42% patients with gallstone pancreatitis. Others have also reported a yield of 37%-42% by ERCP in biliary pancreatitis.30,31 This supports the view that preoperative ERCP may be beneficial in these cases.30 However according to Himal,32 Miller et al33 and Bulkin et al11 preoperative ERCP is not indicated for patients with mild gallstone pancreatitis. Lin et al34 recommend performing a preoperative ERCP only on patients who present with ultrasonographic finding of CBD dilatation. C. de Virgilio et al35 restrict preoperative ERCP to patients with cholangitis, persistent hyperbilirubinemia or persistent hyperamylasemia. According to Canal & Broadie36 laparoscopic cholecystectomy is effective and can be safely performed in patients with acute gallstone pancreatitis. They feel most of these cases can be managed without preoperative ERCP. The optimal management of gallstone pancreatitis and CBD stones, however depends on the skills and resources available as well as patient preference.11 As shown by our results in 33(91.7%) cases ERCP did not demonstrate any calculus in the common bile duct, which in effect means that it was not necessary. This proves the hypothesis that in most instances of gallstone induced pancreatitis, the stones after inducing the attack of pancreatitis pass into the duodenum and are usually not present in the common bile duct. ERCP showed stones in the common duct in 3(8.3%) cases, which had, sonological as well as biochemical (raised AKP and AST) evidence of choledocholithiasis. We advocate the use of precholecystectomy ERCP in follow up cases of gallstone pancreatitis only if there are sonological features suggestive of choledocholithiasis and/or an elevation specifically of alkaline phosphatase and aspartate transaminase in the liver function tests. REFERENCES 1. Bourke JB. Incidence and mortality of acute pancreatitis. BMJ 1977;2:1688-9. 2. Cornfield AP, Cooper MJ, Williamson RC. Acute pancreatitis: a lethal disease of increasing incidence. Gut 1985;26:724-9. 3. Wilson C, Imrie CW. Changing patterns of incidence and mortality from acute pancreatitis in Scotland, 1961-1985. Br J Surg 1990;77:731-4. 4. Thompson SR, Hendry WS, McFarlane GA, Davidson AI. Epidemiology and outcome of acute pancreatitis. Br J Surg 1987;74:398-401. 5. Mann DV, Hershman MJ, Hittinger R, Glazer G. Multicentre audit of death from acute pancreatitis. Br J Surg 1994;81:890-3. 6. De Beaux AC, Palmer KR, Carter DC. Factors influencing morbidity and mortality in acute pancreatitis: an analysis of 279 cases. Gut 1995;37:121-6. 7. Sargen K, Kingsnorth AN. Management of Gallstone Pancreatitis: Effects of Deviation from Clinical Guidelines. Journal of Pancreas-http://www.joplink.net- 2001;2:317-22. 8. Kelly TR. Gallstone pancreatitis: the timing of surgery. Surgery 1980;88:345-50. 9. Paloyan D, Simonowitz D, Skinner DB. The timing of biliary tract operations in patients with pancreatitis associated with gallstones. Surg Gynecol Obstet 1975;141:737-9. 10. Osborne DH, Imrie CW, Carter DC. Biliary surgery in the same admission for gallstone associated acute pancreatitis. Br J Surg 1981;68:758-61. 11. Bulkin AJ, Tebyani N, Dorazio RA. Gallstone pancreatitis in the era of laparoscopic cholecystectomy. Am Surg 1997;63:900-3. 12. Kirchner R, Lausen M, Salm R, Scholmerich J. Acute gallstone pancreatitis. Digestive Surgery 1990;7:1-4. 13. Prince M. Pancreatic apoplexy with a report of two cases. Boston Med Surg J 1882;107:28-55. 14. Opie EL. The relation of cholelithiasis to disease of the pancreas and to fat necrosis. Bullet Johns Hopkins Hosp 1901;12:19-22. 15. Cohen M, Slezak L, Wells C, Anderson DK, Topazian M. Prediction of bile duct stones and complications in gallstone pancreatitis using early laboratory trends. Am J Gastroenterol 2001;96:3305-11. 16. Vogel JD, Yeo CJ. Acute Pancreatitis. Shakelfords' Surgery of the Alimentary Tract. 5th edn. WB Saunders Company; 2002. Vol 3. pp. 9-25. 17. Barkun AN, Barkun JS, Fried GM, Ghitulescu G, Steinmetz O, Pham C, et al. Useful predictors of bile duct stones in patients undergoing laparoscopic cholecystectomy. McGill Gallstone Treatment Group. Ann Surg 1994;220:32-9. 18. Abboud PA, Malet PF, Berlin JA, Staroscik R, Cabana MD, Clarke JR, et al. Predictors of common bile duct stones prior to cholecystectomy: a mete analysis. Gastrointest Endosc 1996;44:450-5. 19. Prat F, Meduri B, Ducot B, Chiche R, Salimbeni-Bartolini, Pelletier G. Prediction of common bile duct stones by noninvasive tests. Ann Surg 1999;229:362-8. 20. Menezes N, Marson LP, deBeaux AC, Muir IM, Auld CD. Prospective analysis of a scoring system to predict choledocholithiasis. Br J Surg 2000;87:1176-81. 21. Alam MK. Assesement of indicators for predicting choledocholithiasis before laparoscopic cholecystectomy. Ann Saudi Med 1998;18:511-3. 22. Santucci L, Natalini G, Sarpi L, Fiorucci, Solinas A, Morelli A. Selective endoscopic retrograde cholangiography and preoperative bile duct stone removal in patients scheduled for laparoscopic cholecystectomy. Am J Gastroenterol 1996;91:1326-30. 23. Robertson GS, Jagger C, Johnson PR, Rathbone BJ, Wicks AC, Lloyd DM, et al. Selection criteria for preoperative endoscopic retrograde cholangiopancreatography in the laparoscopic era. Arch Surg 1996;131:89-94. 24. Carter DC. Special aspects of gallstone pancreatitis. Surgery of the Pancreas. 2nd edn. Churchill Livingstone; 1997. pp. 249-61. 25. Binmoeller KF, Schafer TW. Endoscopic management of bile duct stones. J Clin Gastroenterol 2001;32:106-18. 26. Liu TH, Consorti ET, Kawashima A, Ernst RD, Black CT, Greger PH Jr, et al. The efficacy of magnetic resonance cholangiography for the evaluation of patients with suspected choledocholithiasis before laparoscopic cholecystectomy. Am J Surg 1999;178:480-4. 27. Goodman AJ, Neoptolemos JP, Carre-Locke DL, Finlay DB, Fossard DP. Detection of gallstones after acute pancreatitis. Gut 1985;26:125-32. 28. Lee MJ, Choi TK, Lai EC, Wong KP, Ngan H, Wong J. Endoscopic retrograde cholangiopancreatography after acute pancreatitis. Surg Gynecol Obstet 1986;163:354-8. 29. Tate JJ, Lau WY, Li AK. Laparoscopic cholecystectomy for biliary pancreatitis. Br J Surg 1994;81:720-2. 30. Graham SM, Flowers JL, Scott TR, Bailey RW, Scovill WA, Zucker KA, et al. Laparoscopic cholecystectomy and common bile duct stones. The utility of planned perioperative endoscopic retrograde cholangiography and sphincterotomy: experience with 63 patients. Ann Surg 1993;218:61-7. 31. Buse PE, Edmundowicz SE, Soper NJ, Aliperti G. Management of gallstone pancreatitis with ERCP and laparoscopic cholecystectomy. Gastrointest Endosc 1992;38:292-3. 32. Himal HS. Preoperative ERCP is not necessary in mild gallstone pancreatitis. Surg Endosc 1999;13:782-3. 33. Miller RE, Kimmelstiel FM, Winkler WP. Management of common bile duct stones in the era of laparoscopic cholecystectomy. Am J Surg 1995;169:273-6. 34. Lin G, Halevy A, Girtler O, Gold-Deutch, Zisman A, Scapa E. The role of endoscopic retrograde cholangiopancreatography in management of patients recovering from acute biliary pancreatitis in the laparoscopic era. Surg Endosc 1997;11:371-5. 35. de Virgilio C, Verbin L, Linder S, Stabile BE, Klein S. Gallstone pancreatitis. The role of preoperative endoscopic retrograde cholangiopancreatography. Arch Surg 1994;129:909-13. 36. Canal DF, Broadie TA. Results of laparoscopic cholecystectomy for the treatment of gallstone pancreatitis. Am Surg 1994;60;495-9. © 2003 Indian Journal of Surgery. Also available online at http://www.indianjsurg.com The following images related to this document are available:Photo images[is03106t1.jpg] |
| |||||||||

{kind=link}