 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
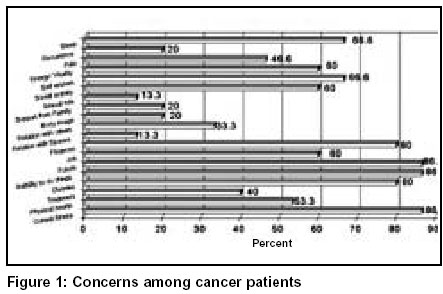
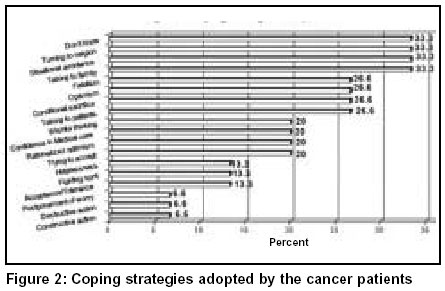
Indian Journal of Surgery, Vol. 65, No. 6, November-December, 2003, pp. 496-499 Concerns and coping strategies in patients with oral cancer: A pilot study Manoj Pandey, P. T. Latha,* Aleyamma Mathew,* K. Ramdas,** Santosh K. Chaturvedi,*** Elizabeth M. Iype, Krishnan M. Nair** Departments of Surgical Oncology, *Epidemiology and **Radiotherapy, Regional Cancer Centre, Medical College PO, Trivandrum - 695011, India; and Department of ***Psychiatry, NIMHANS, Bangalore, India. Paper Received: June 2003. Paper Accepted: August 2003. Source of Support: Nil. How to cite this article: Pandey M, Latha PT, Mathew A, Ramdas K, Chaturvedi SK. Concerns and coping strategies in patients with oral cancer: A pilot study. Indian J Surg 2003;65:496-9. Code Number: is03107 ABSTRACT A quality of life outcome monitoring system for head and neck cancer and reconstructive surgery requires tools that are not only valid but reliably address not only the general health and social factors but also is specific for head and neck cancer. Keeping these in mind Trivandrum Quality of Life Study (TQOLS) was conceived. The pilot study was carried out between April and July 1998. The domains included were psychosocial, sexual, coping, concerns, general health and treatment related factors beside demographic details. The results of this pilot study are reported here. Communication with family, friends and medical persons was most commonly affected followed by withdrawal from social activities. However, most of the patients continued family and religious activity. Similarly turning to religion was the most common coping mechanism among 80% of the patients. In majority of patients this was the first coping mechanism. As the numbers of patients in the present study are limited the results cannot be generalized. However, we presume that they will act as a guide for the main study. Key words: Head neck cancers, Oral cavity, Quality of life, Coping, Concerns, Pain, Psycho-oncology, Anxiety, Depression, Functions. INTRODUCTION Cancer affects about 300,000 people each year in India. Cancer of the head and neck effects some of the most fundamental life functions including airway, digestion, deglutition and speech. Advances in the cancer treatment have brought about significant increase in survival for the patients with variety of malignancies. Aspects of cancer treatment beyond prolonging the survival have emerged with a focus on quality, not just quantity, of survival through the identification of psychosocial needs.1,2 Assessment of psychosocial aspects of the disease process and its treatment is integral in evaluating individual quality of life issues.3 These QOL assessment has been used in research and clinical practice to characterize the burden created by cancer and / or its treatment, select treatment options, demonstrate the effect of rehabilitative approaches and for policy decisions.4-6 Once QOL measures the vulnerable period and factors, interventions can be directed to them. The quality of survival after treatment for head and neck cancer patient is an important consideration for evaluation of treatment and rehabilitation outcome. Increased survival rates dictate that quality of life, as well as disease control and length of survival can be a measure of cancer treatment efficacy.7 The subjective evaluation of persons psychological well being should be measured in conjunction with objective data that determine treatment outcome for head and neck cancer. The various scales used to measure QOL range from global measures like Karnofsky's performance status,8 Activity of daily living (ADL) and Linear Analogue Scale for Self Assessment (LASA), to specific quality of life scales like Quality of Life Index (QLI), QLI short form (QLI-SF), Functional Assessment of chronic illness and treatment (FACT), Eastern Cooperative Oncology Group (ECOG) scale etc. Beside general health, family, and psychosocial factors coping, concerns and above all the functional status influences the QOL outcome.7,9-11 We carried out this study to evaluate the economic, demographic, psychosocial factors, coping, concerns and functional status on quality of life among patients with head and neck cancer. MATERIAL AND METHODS Trivandrum Quality f Life Study (TQOLS) was started in April 1998 and the pilot was completed in July 1998. For this study 15 patient with head and neck cancers admitted to Surgical Oncology ward for primary surgery were included. All measurements were made in preoperative patients, either a day or two before surgery as per the patient convenience. Specially developed TQOLS questionnaire recorded the personal and demographic details, psychosocial factors, concerns, coping and functional assessment. The questionnaire was based on the informal patient interviews, literature search and discussions with experts in this field. The questionnaire was not previously validated. An investigator trained in carrying out the patient interviews (PTL) carried out the interviews. The interviewer was not the part of treatment team. Frequency tables were produced using Epi-info 5 statistical software and the data is presented in percentages. RESULTS Mean age of the patients was 54 years ranging from 35 to 65 years. The male to female ratio was 4:1. Sixty percent of our patients were Hindus, 20% Muslim and 13% Christians. All the 15 patients were married and had families. Forty six percent had only primary education, 26.6% high school, while 26.6% had no formal education. Similarly 53.3% of the spouses had primary education, 13.3% high school and 5 had no formal education, all the patients and spouses were able to write their names. Most of our patients were agriculturists (33.3%), 20% were laborers, 13.3 % fishermen and 20% were in some other occupations while 13% were unemployed. All the patients had a family income < 1000/- Rupees with more than three family members. Majority of the patients (80%) owned land and the rest were landless. The most common social problem faced by the patients was difficulty to tell others (60%), 40% told that they are shy meeting people, 33.3% hid their diagnosis from family and friends. The children of 46.6% were married at the time of the diagnosis among rest only one patient had problem getting his child married. Majority of the patients (80%) participated in family functions of which 75% continued to do so as before. Similarly 80% regularly participated in religious functions of which only 58.3% continued in the same fashion after treatment. Participation in social functions was only in 53.3% of which 62% participated as before. The biggest handicap was recreational activities, which were present only in 13.3% patients, and these patients too indulged in these activities rarely (Figure 1). Attitude of children towards their parents with cancer was sympathetic in 60%, Over protective in 20%, and understanding in 7%. Current illness, inability to do things of their own and future were the biggest concerns in 86.6% patients, 80% patients were disturbed or upset, loss of self esteem and sleep disturbances were seen in 66.7%. Duty as a parent, dependence on others affected QOL in 53.3% while social activities, energy and vitality was effected in 60%. Relations with spouses, relations with others, family support and sexual role was of concern in only 13-20% patients (Figure 1). Almost 80% of the patients felt that more information will help to decrease anxiety, 53% felt that this is a punishment for their past deeds, 33% had difficulty in expressing to medical persons while 13% felt the disease is contagious. Biggest worry of patients was duty as parent in 46.6%, job and financial security in 30% and future concerns in 6.67%. Turning to religion was the commonest coping mechanism in 53.3% followed by talking to family and friends in 33.3%, situational avoidance in 33.3%, talking to other patients in 26.6%, conditional sacrifice and optimism was seen in 26.6% while fatalism was present in 26.6%. Among a small number of patients acceptance and confidence in medical care and wishful thinking (20%) were also seen. The first coping mechanism in majority was turning to religion, followed by optimism, talking to friends and family and situational avoidance (Figure 2). Among the functional status shoulder mobility was restricted in 33.3%, difficulty in chewing was present in 46.7%, difficulty in swallowing in 13.3%, absence of taste in 33.3%, dry mouth in 20%, eating problems were seen in 53.3%. Change in appearance was felt by 20%, pain was present in 46.7% and fatigue in 33.3%. All the patients were prescribed analgesics for pain but none took it regularly. The disease interfered with normal routine in 53.3%, social and sex life in 33.3% each, housework in 46.7% while 33.3% had poor concentration at work. Almost half (53.3%) patients rated there past week as satisfactory while 33.3% said it was unsatisfactory. DISCUSSION Quality of life is a complex concept that is associated with multiple domains. Various domains included are economic, family, friendship, age, home, community, and indicators of physical health and functional status.7 Of all identified domains physical health has been shown to have the greatest impact on overall quality of life.12-13 Due to preliminary nature of the present study it was not possible to find the effect of various domains on overall quality of life. However, the most affected domains in the present study were communication with family, friends and medical personals social withdrawal, withdrawal from recreational activities, current illness and inability to do things. Most of these are part of general health and psychosocial domains. On the other hand the family relations and spiritual domains remain unchanged. A global QOL measure was not used in this study as it was thought that most of the domains in global QOL are covered by the present questionnaire. The commonest coping mechanism was turning to religion followed by talking to family and friends, situational avoidance and talking to other patients. Coping refers to the thoughts and acts used by and individual to manage the internal or external demands or both that tax or exceed his or her psychological resources.11-14 The coping is conceived as a dynamic process dependent on the person environment transaction.10 In our series confidence in treatment and medical persons was seen as a coping mechanism in a small number of patients. Functional disability was seen among a small number of patients. Pain was a limiting factor in 50% patients in our series. All the patients were prescribed the analgesics as per the WHO ladder, however, only one patient regularly took the prescribed analgesics. Most important factor coming out of this preliminary study is regarding concerns. It was observed that majority of the patients were not concerned about their disease and treatment outcome, however, they were worried regarding their duty as parent (seen only in patients with young unmarried children), finances, job security and future of their families. These findings were in contrast to what was earlier observed and perceived in western studies. Due to small number of patients and preliminary nature of the present report not much emphasis can be laid on to the results. However, these results have guided us to carry forward and press for modifications in the main "Trivandrum Quality of Life Study". The biggest difficulty was that the questionnaire was too bulky and used to take about 90 minutes to complete, hence for most patients it was not possible to concentrate that long. Some of the patients had difficulty in understanding some of the questions. Hence the two main modifications are in form of shortening of questionnaire and modification of items. It further shows the need to develop indigenous QOL Scales and inventories and the need for more scientific prospective studies in this area. Longitudnal studies on QOL and coping may help understanding the process better and will help in ultimately improving the QOL of these patients. REFERENCES 1. Groenwald SL, Frogge MH, Goodman M, Yarbro CH, editors. Cancer Nursing: principles and practice. Boston: Jones and Barlett Publishers; 3rd edn. 1993. 2. Lee CS. Quality of life and breast cancer survivors. Psychosocial and treatment issues. Cancer Practice 1997;5:309-16. 3. Aaronson NK. Methodological issues in assessing the quality of life of cancer patients. Cancer 1990;67:844-50. 4. Aaronson NK, Meyerowitz BE, Bard M, Bloom JR, Fawzy FI, Feldstein M, et al. Quality of life research in oncology. Past achievements and future priorities. Cancer 1991;67: 839-43. 5. Bloom JR. Quality of life after cancer. Cancer 1990;67:655-9. 6. Grant M, Padilla GV, Ferrell BR, Rhiner M. Assessment of quality of life with a single instrument. Semin Oncol Nursing 1990;6: 260-70. 7. Baker C. A functional status scale for measuring quality of life outcomes in head and neck cancer patients. Cancer Nursing 1995;18:452-7. 8. Karnofsky DA, Burchenal JH. Clinical evaluation of chemotherapeutic agents in cancer. In: Macleod CM, editor. Evaluation of chemotherapeutic agents. New York: Columbia Press; 1949. pp. 191-205. 9. Gliklich RE, Goldsmith TA, Funk GF. Are head and neck specific quality of life measures necessary? Head Neck 1997;19: 474-80. 10. Lazarus RS, Folkman S. Stress appraisal and coping. New York, Springer 1984. 11. Callen VJ, Hennessey JF. Strategies for coping with infertility. Br J Med Psychol 1989;62:343-54. 12. Campbell A, Converse PE, Rodgers WL. The quality of American life. New York, Russel sage Foundation 1976. 13. Andrews F, Withey S. Social indicators of well being. New York, Plenum 1976. 14. Folkman S, Lazarus RS. Stress process and depressive symptomatology. J Abnormal Psychol 1986;95:107-13. © 2003 Indian Journal of Surgery. Also available online at http://www.indianjsurg.com The following images related to this document are available:Photo images[is03107f1.jpg] [is03107f2.jpg] |
| |||||||||

{kind=link}
{kind=link}