 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
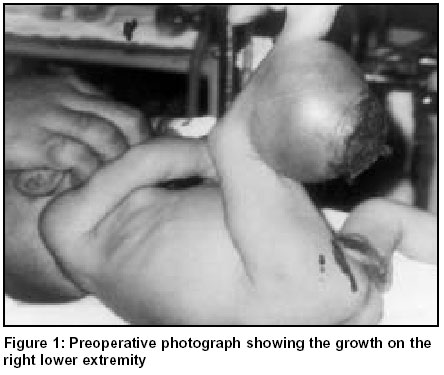
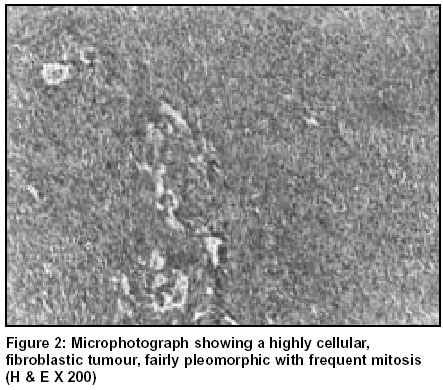
Indian Journal of Surgery, Vol. 65, No. 6, November-December, 2003, pp. 510-511 Case report Congenital fibrosarcoma: A case report with review of literature Pramod Kumar Gonda 33, Park Enclave, Northern Town, Jamshedpur - 837001, India. Paper Received: January 2002. Paper Accepted: September 2002. Source of Support: Nil. How to cite this article: Gonda PK. Congenital fibrosarcoma: A case report with review of literature. Indian J Surg 2003;65:510-1. Code Number: is03110 ABSTRACT We report a case of congenital fibrosarcoma, an unusual childhood tumour, and review the relevant literature. These tumours occur in children under 5 years of age, and about 300 cases are reported in the literature. However, only a few of them are present since birth. Key words: Congenital, Fibrosarcoma, Extremity. INTRODUCTION Congenital fibrosarcoma is a rare soft tissue malignancy involving the extremities. Histologically, they are similar to their adult counterparts but differ in their clinical behaviour. Though recurrence is common, metastases are rare and prognosis is good. There are only three cases of childhood fibrosarcoma reported from the Indian subcontinent. We report a case of congenital fibrosarcoma of the lower extremity in a 7-day-old male infant. The case was followed up for 2 years without any recurrence or metastases. CASE REPORT A 7-day-old male infant was noticed to have a painless ulcerated swelling over the right leg since birth. The mother had a prolonged and difficult labour due to the mass. The baby was treated with antibiotics and local dressings but failed to show improvement. The baby was brought to the hospital due to rapid growth of the tumour and bleeding. On examination, a hard mass of 11 cm X 9 cm, with shining skin, prominent blood vessels and central ulceration, was seen over the right calf region (Figure 1). X-ray of the leg showed the soft tissue mass. Doppler ultrasonography revealed a solid mass with gross vascularity. The mass was situated between the calf muscles and was away from the bone. Excision of the mass was undertaken with ligation of the feeding vessels. Postoperative recovery was uneventful with primary healing; the vascularity of the foot was not compromised. Histopathological examination showed the tumour to be a poorly circumscribed, fibromatous mass measuring 8 X 5 X 4 cm, soft to firm in consistency with greyish white cut surface with areas of haemorrhage and necrosis. It was highly cellular with fibroblastic proliferation. Pleomorphic spindle-shaped cells separated by variable amounts of collagen were present. Frequent mitosis was seen with scattered lymphocytes (Figure 2). Reticulin stain showed fibres around individual tumour cells. Immunohistochemically, the cells were strongly positive for vimentin (tumour marker for cells of mesenchymal origin) and negative for desmin (tumour marker for smooth muscles), supporting the diagnosis of fibrosarcoma. DISCUSSION Paediatric soft tissue sarcomas account for 7% of all childhood tumours. Congenital fibrosarcoma is a rare soft tissue malignancy, and 300 cases have been reported in the world literature.1 The age groups affected are infants and young children under the age of five (congenital variety), and children between 10 and 15 years of age.2 These tumours originate from the primitive mesenchymal tissue. The common sites are the trunk and the extremities. There is no evidence of increased familial incidence but chromosomal analysis has revealed a non-random gain of extra chromosomes, +8, +11. +17, +20 and an abnormal karyotype 48,XY, 11 and 20.4 These tumours affect children under the age of five with a slight male preponderance. Clinically, they present with a rapidly enlarging swelling in the soft tissue. Commoner sites of involvement are the extremities, head, neck, trunk, and retroperitoneum. They may be asymptomatic initially or may show symptoms because of local invasion. The local complications include ulceration, haemorrhage and infection. These tumours are rapid-growing and are known to attain large sizes. Histologically, the tumours bear a close resemblance to fibrosarcoma in adults, having anaplastic spindle-shaped cells arranged in a herring bone pattern, however, some of the striking features are—uniform, well-oriented fibroblasts, scattered round cells, and chronic inflammatory cells like lymphocytes. Multinucleated giant cells are rare. Mitotic figures are a common feature. Rich vascular areas may be seen. The tumour needs to be distinguished from the richly cellular but benign form of fibromatosis and other types of soft tissue sarcomas like embryonal rhabdomyosarcoma, synovial sarcoma and neurofibrosarcomas. Treatment is wide local excision or amputation. Chemotherapy and radiotherapy are reserved for unresectable tumours and for recurrences or metastases. Congenital fibrosarcoma has an excellent prognosis. Chung and Enzinger reported a 5-year survival rate of 84% in a series of 53 cases.3 There are higher metastatic and mortality rates for axial lesions, indicating a more aggressive behaviour. The relatively benign course of such tumours may be due to two factors—a significantly lower proliferative index coupled with enhanced apoptosis. The favourable clinical course and biological features of congenital_infantile sarcomas have raised a question about its nomenclature as sarcoma rather than a borderline tumour.4,5 This case did not have a recurrence or any metastasis in its follow-up period of 2 years. ACKNOWLEDGEMENTs We express our sincere thanks to Dr. M. N. Bhat, Chief of Medical Services for his valuable opinion and permission for publishing this article. REFERENCES 1. Enzinger FM, Sharon WW. Congenital & infantile fibrosarcoma. Soft Tissue tumours 1983;115-22. 2. Schofield DE, Flether JA, Grier HE, Yunis EJ. Fibrosarcomas in infants & children. Application of new techniques. Am J Surg Pathol 1994;18:14-24. 3. Chung EB, Enzinger FM, Infantile fibrosarcoma. Cancer 1976;38:729-39. 4. Wilson MB, Stanley W, Sens D, Garvin AJ. Infantile Fibrosarcoma-a misnomer? Paed Pathol 1990;10:901-7. 5. Coffin CM, Jaszoz W, Oshea PA, Dehner LP. So called infantile fibrosarcomas. Does it exist and what is it? Paed Pathol 1994;14:133-50. © 2003 Indian Journal of Surgery. Also available online at http://www.indianjsurg.com The following images related to this document are available:Photo images[is03110f2.jpg] [is03110f1.jpg] |
| |||||||||

{kind=link}
{kind=link}