 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 65, No. 6, November-December, 2003, pp. 513-514 Gastrointestinal lipomas presenting as obstruction Harsh Mohan, Amanjit Bal Department of Pathology, Govt. Medical College & Hospital, Sector - 32-A, Chandigarh, India. Paper Received: June 2002. Paper Accepted: December 2002. Source of Support: Nil. How to site this article: Mohan H, Bal A. Gastrointestinal lipomas presenting as obstruction. Indian J Surg 2003;65:513-4. Code Number: is03112 ABSTRACT Lipomas are benign tumours common at other sites but rare in the gastrointestinal tract. The colon is the commonest location for lipomas in the gastrointestinal tract, but gastric and duodenal lipomas are rare. Most of the lipomas are clinically silent but rarely they can present with bleeding or obstruction. Large lipomas causing obstruction can mimic malignant tumours clinically as well as on endoscopy. To rule out malignant lesion and avoid extensive surgical procedures biopsy or intraoperative frozen section is a must. Key words: Lipoma, Gastrointestinal, Obstruction. INTRODUCTION Gastrointestinal (GI) lipomas are benign, slow-growing tumours constituting only 5-6% of GI tumours. In the GI tract their most common location is the colon, accounting for 60-75% of all GI lipomas,1 followed by the small intestine (20-25%).2 Duodenal and gastric lipomas are rare. The stomach accounts for 5% of all GI lipomas.3 To date, only about 200 gastric lipomas have been described in world literature.4 GI lipomas are usually asymptomatic but rarely can present with obstruction or GI bleeding. We report three cases of GI lipomas presenting as obstruction. CASE REPORTS Case 1
Case 2
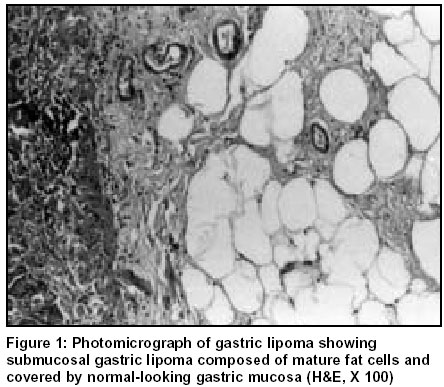
Case 3 DISCUSSION Lipomas are benign tumours that are common in other sites but rare in the GI tract. In the GI tract they are mainly located in the colon. Gastric lipomas constitute 3% of all gastric tumours with 75% of them located in the antrum.5 Most of the GI lipomas are submucosal in origin, only 5% are subserosal in origin.6 GI lipomas are generally asymptomatic and the tumour size and location usually dictates the occurrence of symptoms. Lipomas less than 1 cm in size are usually asymptomatic but lesions greater than 4 cm become symptomatic and present with GI bleeding from ulceration of the overlying mucosa or rarely with symptoms of obstruction and intussusception.7 The GI lipomas can be diagnosed by GI endoscopy which is the preferred modality for small lesions. The endoscopic findings which are positive predictors of benign lesions are: a sharply defined submucosal mass, often yellow in colour as opposed to the surrounding pink mucosa. Sometimes, clinically it is difficult to make a distinction between GI lipomas and other intramural tumours like leiomyoma, leiomyosarcoma, adenomyoma and fibroma, especially when the size of the tumour is large. In such cases endoscopic ultrasonography8 and CT scan can be of help but confirmatory diagnosis is made on histological examination only. Incisional biopsy can be performed in large lesions to rule out malignancy. The treatment of choice for symptomatic GI lipoma is local enucleation or cicumferential excision with a clear margin of normal tissue. GI lipomas are benign tumours and do not have potential for malignant transformation, so intraoperative frozen section and histological diagnosis is essential to rule out malignant lesions and avoid extensive surgical procedures such as extended gastrectomy and colectomy. REFERENCES 1. Alberti D, Grazioli L, Orizio P. Asmyptomatic giant gastric lipoma: what to do? Am J Gastroenterol 1999:94;3634-7. 2. Agha FB, Dent TL, Fiddian Green RG. Bleeding lipomas of upper gastrointestinal tract. A diagnostic challenge. Am Surg 1985:51;279-85. 3. Maderal F, Hunter F, Fuselier G. Gastric lipomas- an update of clinical presentation, diagnosis and treatment. Am J Gastroenterol 1984:79;964-7. 4. Antes G, Neher M. Lipoma of the stomach- diagnosis and therapy. Rontegenpraxis 1995:48;252-3. 5. Ciraldo A, Thomas D, Schmidt S. Gastric lipoma presenting as gastrointestinal bleeding-a case report. Internet J Oncol 2000:1. 6. Myint M, Atten MJ, Attar BM. Gastric lipoma with severe haemorrhage. Am J Gastroenterol 1996:91;811-12. 7. Patankar T, Prasad S, Patankar Z, Chaudary S. Ileo-colic intussusception secondary to ileal lipoma. JAPI J Assoc Physicians India 1999;47:923-5. 8. Kameyama H, Niwa Y, Arisawa T, Goto H, Hayakawa T. Endoscopic ultrasonography in the diagnosis of submucosal lesions of large intestine. Gastrointest Endosc 1997;46:406-11. © 2003 Indian Journal of Surgery. Also available online at http://www.indianjsurg.com The following images related to this document are available:Photo images[is03112f1.jpg] |
| |||||||||

{kind=link}