 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
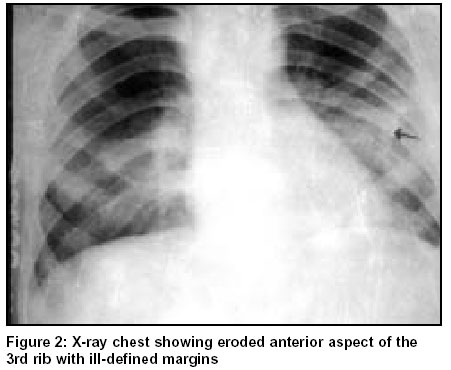
Indian Journal of Surgery, Vol. 65, No. 6, November-December, 2003, pp. 515-516 Tuberculous osteomyelitis: A bizarre presentation Paras R Kothari, Tarun Kumar, Ashish Jiwane, Bharati Kulkarni, Alka Kalgutkar Department of Paediatric Surgery, L.T.M. Medical College and General Hospital, Sion, Mumbai - 400022, India. Paper Received: October 2001. Paper Accepted: January 2002. Source of Support: Nil. How to cite this article: Kothari PR, Kumar T, Jiwane A, Kulkarni B, Kalgutkar A. Tuberculous osteomyelitis: A bizarre presentation. Indian J Surg 2003;65:515-6. Code Number: is03113 ABSTRACT An 11-year-old boy presented with multiple swellings all over the body. One of the swellings present over the chest was incised and drained. This revealed the diagnosis by the demonstration of tubercle bacilli in the discharge from cutaneous sinuses and cold abscesses. Surgical treatment was followed by four-drug anti-tubercular chemotherapy. Key words: Tuberculosis, Osteomyelitis. INTRODUCTION Tuberculosis involving multiple sites and occurring without evidence of a primary focus is rare.1 It is unusual to encounter tuberculosis of flat bones of the skull in infants and children. Specific anti-tubercular chemotherapy should suffice as treatment for early lesions. If there is lack of response to treatment or in the presence of complications, surgery is necessary. We report a case of multiple sites of tuberculosis without any evidence of primary foci, which is rare. CASE REPORT An 11-year-old boy presented with swellings on the chest wall, left knee and right ankle. He had low-grade fever with evening rise of temperature for 1½ months. Two swellings had appeared on the chest wall within a span of 15 days. On examination the swellings were 5 x 4 cm and 2 x 2 cm on the right side of the sternum at the 3rd -4th costo chondral junction. Both the swellings were smooth-surfaced, non-tender and fluctuant. The left knee joint swelling appeared 15 days later and was associated with pain and restricted movements. The right ankle joint had minimal swelling with pain but the movements were unrestricted. No history of trauma could be elicited. Investigations showed an erythrocyte sedimentation rate of 105 mm at end of the 1st hour and an eosinophilia of 14 %. The Mantoux test was positive. Rheumatoid arthritis factor was negative. X-ray of the chest (Figure 1) showed erosion of the anterior aspect of the 3rd rib with ill-defined margins. X-ray of the skull (Figure 2) showed multiple lytic lesions without sclerosis in the parietal and occipital regions. X-ray left knee joint showed a lytic lesion in the distal tibial epiphysis and medial malleolus. Irregularity of cortical material and decreased density of bones and soft tissue swelling was also seen. Ultrasonography of chest showed hypoechoeic lesions suggestive of a cold abscess with underlying rib erosion. Ultrasonography of the left knee joint showed mild to moderate effusion with synovial thickening. Wassermann and Kahn tests were negative and examination of the faeces showed no evidence of intestinal parasites. Under general anaesthesia, the infective chest swellings were drained. Pus and granulation tissue showed acid-fast bacilli on Ziehl_Neelsen staining. The wound was closed in two layers. Histopathology of the lesion showed chronic inflammatory granulation tissue with foreign body type giant cells and epithelial granuloma and caseation. Anti-tubercular chemotherapy was started. Examination of the sputum failed to produce any further evidence of tuberculosis. He was discharged 4 weeks after admission when the chest wound showed signs of healing. The knee joint swelling had also decreased and the patient was afebrile. Follow-up of the patient after 2 months of discharge showed some remineralization of the skull bone. DISCUSSION A decline in the incidence of tuberculosis has resulted from improvement of living standards. This is seen more in the western world than in the developing countries. But with more cases of AIDS, tuberculosis is once again emerging as a clinical entity. Skull tuberculosis is rarely encountered in children.2 Calvarian tuberculosis accounts for less than 0.2% of all types of bone diseases. Radiographically, tubercular osteomyelitis resembles non-specific osteomyelitis.3 The first demonstrable change is a small area of translucency due to decalcification. At this stage the lesion is undetectable on clinical examination. As the lesion progresses the area of decalcification increases in size and bone destruction occurs. If there is progressive infiltration the translucency spreads in an irregular fashion. The speckled density, i.e., bone sand or actual sequestra may be visible. Similar radiological findings occur in (a) eosinophilic granuloma (multiple cystic lesions associated with seborrhea, mild generalized adenopathy and hepatomegaly) (b) congenital syphilis (associated with severe syphilitic osteitis of the long bone), and (c) secondary deposits or malignancy.4 Alcohol-fast and acid-fast bacilli is seldom detected in the aspirated pus, but frequently, secondarily infecting organisms have been seen and cultured. Histology of the granulation material is a better means of confirming the diagnosis. It has been suggested that trauma plays a major role in skeletal tuberculosis. In our case there was no history of trauma.5 Specific anti-tubercular chemotherapy should suffice as treatment for early lesions. In case of lack of response to treatment or in the presence of a mass, surgery is necessary. The object of the operation should be to remove badly affected bones together with any sequestra and a substantial amount of the granulation tissue. In modern circumstances of effective anti-tuberculosis chemotherapy, surgery need not be very radical.6 Fulminating secondary infection would also seem to indicate the need for surgery. Diagnosis of tuberculosus should be entertained in the absence of trauma and when sinuses, a positive tuberculin test and a high erythrocyte sedimentation rate are present along with negative serology test for syphilis. Demonstration of tubercle bacilli by staining or culture or biopsy of bone and granulation tissue, is necessary for further confirmation of tuberculosis. We strongly recommend anti-tubercular treatment for a period of one-and-a-half year even in such severe bony involvement 7 once diagnosis is established. REFERENCES 1. Rajeshwari K, Sharma A. Multifocal skeletal tuberculosis presenting as osteitis skull and atlantoaxial dislocation. Ind Paediatr 1995;32:1214-9 2. Caffey J. Pediatric X-ray diagnosis. 6th edn. Chicago: Year book medical Publishers; 1979. pp. 79 3. Ridley N, Shaikh MI, Remedios D, Mitchell R. Radiology of Skeletal Tuberculosis. Orthopedics 1998;21:1213-20. 4. Bhandari B, Mandowara SL, Joshi H. Tubercular Osteomyelitis of skull. Indian J Paediat 1981;48:113-5. 5. Davidson PT, Horowitz I. Skeletal tuberculosis. Am J Med 1970;48:77-84. 6. Miles J, Hughes B. Tuberculous osteitis of the skull. Br J Surg 1970;57:673-9. 7. Mohanty S, Rao CJ, Mukherjee KC. Tuberculosis of the skull. Int Surg 1981;66:81-3. © 2003 Indian Journal of Surgery. Also available online at http://www.indianjsurg.com The following images related to this document are available:Photo images[is03113f2.jpg] [is03113f1.jpg] |
| |||||||||

{kind=link}
{kind=link}