 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
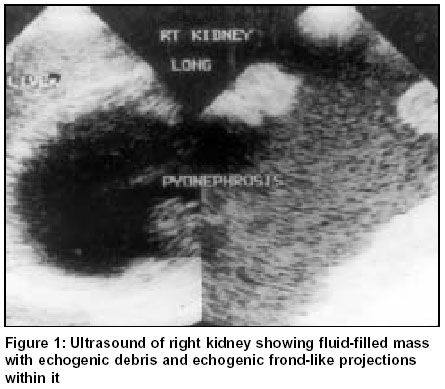
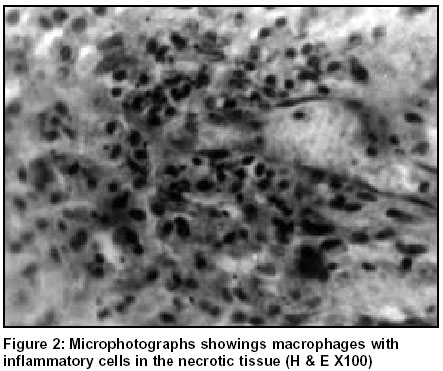
Indian Journal of Surgery, Vol. 65, No. 6, November-December, 2003, pp. 517-518 Xanthogranulomatous pylonephritis: An unusual presentation Dilip Kumar Pal, Samiran Samanta,* Tusar Kanti** Departments of Urology *Radiology and **Pathology, Bankura Sammilani Medical College, Bankura, West Bengal - 722102, India. Paper Received: September 2002. Paper Accepted: February 2003. Source of Support: Nil. How to cite this article: Pal DK, Samanta S, Kanti T. Xanthogranulomatous pylonephritis: An unusual presentation. Indian J Surg 2003;65:517-8. Code Number: is03114 ABSTRACT Xanthogranulomatous pylonephritis is a rare, chronic severe renal infection. We report an unusual case of xanthogranulomatous pylonephritis associated with pelvi-ureteric junction obstruction without any renal calculus. Key words: Pylonephritis, Xanthogranulomatous. INTRODUCTION Xanthogranulomatous pylonephritis is a rare entity usually associated with calculi. Proper preoperative diagnosis and therapy pose a challenge to the clinician. This case presented with gross renal destruction associated with pelvi-ureteric junction (PUJ) obstruction without any renal calculi, which is very unusual. CASE REPORT A 34-year-old man presented with a slow-growing swelling and dull aching pain in the right flank for last one year. On examination he had a hugely enlarged, cystic swelling occupying the right half of the abdomen. On investigation he was moderately anaemic with normal renal biochemistry. Ultrasonography showed a grossly enlarged, multiloculated, cystic swelling having thick irregular septa and echogenic debris with echogenic frond-like projections within it (Figure 1). The right ureter was normal. Urography demonstrated non-visualisation of the right kidney with normal pelvi-calycial pattern of the left side. On exploration the right kidney was hugely enlarged pushing the liver upwards and extending up to the lower level of the right iliac fossa. It was strongly adherent with the posterior abdominal wall. The kidney tissue was grossly destroyed and contained haemorrhagic fluid. Nephrectomy, with removal of all the granulomatous tissue was undertaken. The PUJ was stenosed with gross dilatation of the pelvic. On sectioning, the kidney tissue was found to be replaced with a fluid-filled sac with frond-like projections of necrotic tissue within. Culture of the fluid showed growth of proteus. Histology suggested clusters of macrophages with inflammatory cells and extensive necrosis (Figure 2), consistent with xanthogranulomatous pylonephritis. DISCUSSION Xanthogranulomatous pylonephritis is an atypical form of chronic pylonephritis characterized by diffuse, focal or segmental supportive destruction of renal parenchyma and presence of granulomata, abscess and masses of lipid-laden foam cells.1 The disease usually presents with unilateral flank pain, fever, bacteriuria with concurrent or previously treated renal calculi.2 Generally, the infection is caused by proteus or E. Coli. Urography usually reveals renal calculi with poor or absent renal function with ill-defined outline due to spread of infection. CT scan often shows replacement of renal parenchyma with multiple water density areas representing dilated calyces and abscess cavities filled with varying amounts of pus or debris. CT is of special value to note the retroperitoneal and adjacent organ involvement and to differentiate it from renal neoplasm. The present case is unusual due to the absence of fever, sterile urine culture without any renal calculi and associated uretero-pelvic junction obstruction. In advanced cases nephrectomy gives the only hope of cure, which sometimes may be very difficult due to extension of granuloma to the retroperitonium, bowel or great vessels. Great care should be taken to remove the entire granuloma as in most cases it is infected. REFERENCES 1. Schaffer J. Infection of the urinary tract. In: Walsh PC, Retic BA, Stamey TA, Vaughan ED, editors. Campbell' Urology. 6th edn. Pheladelphia: WB Saunders; Vol 1. 1992:731-86. 2. Sanzgiri MD, Rangnekar NP, Mahajan AD, Mahajan RV, Pathak HR. Xanthogranulomatous pylonephritis. An unusual presentation. Detailed analysis of 29 cases and a brief discussion of atypical presentation. Ind J Urol 1999;152-3. © 2003 Indian Journal of Surgery. Also available online at http://www.indianjsurg.com The following images related to this document are available:Photo images[is03114f1.jpg] [is03114f2.jpg] |
| |||||||||

{kind=link}
{kind=link}