 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 66, No. 1, Jan-Feb, 2004, pp. 19-27 Prevention of burst abdominal wound by a new technique: A randomized trial comparing continuous versus interrupted X-suture Anurag Srivastava, Swapandeep Roy, K. B. Sahay,* Vuthaluru Seenu, Arvind Kumar, Sunil Chumber, Sabyasachi Bal, Sadanand Mehta Department of Surgical Disciplines, All India Institute of Medical Sciences; *Department
of Bio-Medical Engineering, Indian Institute of Technology, Delhi, India.
Paper Received: June 2003. Paper Accepted: January 2004. Source of Support: Nil. Code Number: is04005 Abstract Background: Abdominal wound dehiscence is a common complication of emergency
laparotomy in Indian setup. It's prevention is important to reduce post operative
morbidity and mortality
Key Words Abdominal wound dehiscence, Burst abdomen, Suture technique, Randomized trial, Logistic regression, Emergency laparotomy. How to cite this article: Srivastava A, Roy S, Sahay KB, Seenu V, Kumar A, Chumber S, Bal S, Mehta S. Prevention of burst abdominal wound by a new technique: A randomized trial comparing continuous versus interrupted X-suture. Indian J Surg 2004;66:19-27. INTRODUCTION Wound dehiscence carries with it a substantial morbidity. In addition there is an increase in the cost of care both in terms of increased hospital stay nursing and manpower cost in managing the burst and its complications. Many patients in India have a poor nutritional status and the presentation of patients with peritonitis is often delayed in the emergency. This makes the problem of wound dehiscence more common1 and graver in our setting as compared to the West. Wound dehiscence is related to the technique of closure of abdomen and the suture used.1 Numerous studies have been conducted evaluating a bewildering variety of closure techniques and suture materials.2-4 The current opinion in the West centers around some form of running mass closure of the abdomen in both emergency and elective settings as there is no significant difference reported between the two, in most studies.5-13 While the choice may not be so important in elective patients who are nutritionally adequate, do not have any risk factor for dehiscence and are well prepared for surgery, however it may prove crucial in emergency patients who often have multiple risk factors for developing dehiscence14 and the strangulation of the sheath is the proverbial last straw in precipitating wound failure. A new "Interrupted X technique" was developed in our department to circumvent the problem of cutting out effect of a continuous suture. Its clinical usefulness was tested in a randomized trial of midline laparotomy wound closure. MATERIAL AND METHODS A total of 210 patients presenting to either the Casualty Department for emergency laparotomy or through the Surgical wards for elective laparotomy were enrolled in this study. Of these 100 patients were entered in the emergency group and 110 in the elective laparotomy group. The study period ranged from December 1998 to October 2000. The setting was the general surgical wards of AIIMS Hospital. The study was approved by the faculty of the Department of Surgical Disciplines and the Dean's Research Protocol Committee of our Institute. Inclusion Criteria All patients scheduled to undergo a midline laparotomy for emergency or elective reasons. Patients with the following characteristics were not included in the study. Exclusion Criteria
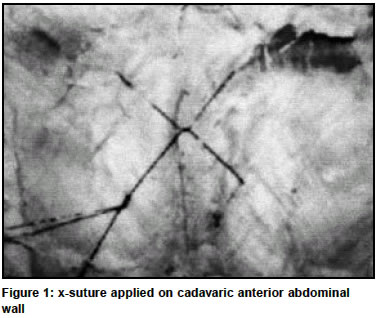
All patients were given explanation of the study and signed a written consent form. They were randomized to undergo either continuous or interrupted closure of the laparotomy incision. The randomization codes determined by a table of random numbers were kept in sealed numbered envelopes which were opened once a patient was deemed suitable for inclusion in the study. A stratified randomization method was used-the two strata comprising emergency and elective laparotomies. In each stratum simple random sampling was utilized for all consecutive eligible patients undergoing laparotomy. We followed Zelen's method15 of taking written informed consent after randomization to a group. Continuous closure was performed using No. 1 Prolene suture (Polypropylene; Ethicon), care being taken to place each bite 1.5 to 2 cm from the linea alba edge and successive bites being 1 cm from each other. The edges of linea alba were gently approximated without strangulation with an attempt to keep a suture to wound length ratio of 4:1.The closure was performed by a Consultant or by a Senior Registrar. Interrupted closure was performed using No. 1 Prolene suture, as shown in Figure 1. A large bite was taken outside-in, 2 cm from the cut edge of linea alba. The needle emerged on the other side from inside out diagonally 2 cm from the edge and 4 cm above or below the first bite. This strand was crossed or looped around the free end of suture (Figure 1) and continued outside-in, diagonally at 900 to the first diagonal. The two ends were tied just tight enough to approximate the edges of linea alba taking care not to include bowel or omentum between the edges. This created two X like crosses-one on the surface and another deep to linea alba. The next X- suture was placed 1 cm away from the previous one. Thus in a 14 cm long wound 3 X-sutures were applied. Each patient was followed for 4 weeks after surgery to determine the risk of dehiscence. Measurement of Variables The main outcome variable was presence of an abdominal wound dehiscence or burst. This was recorded as a binary variable-present/absent. A burst was considered present, when intestine, omentum or other viscera were seen in the abdominal wound. Its presence was ascertained by a consultant surgeon. The following predictor variables were recorded:
Statistical Analysis The following statistical analyses were carried out
RESULTS A total of 210 patients were enrolled in the study - 100 patients in the emergency group and 110 patients in the elective group. Emergency Laparotomy Group There were a total of 100 patients in this group with 25 females and 75 males. The average age of the total sample was 38.06 with a median age of 32 and a standard deviation of 15.209. The age range was from 18 years to 75 years. One patient died soon after the operation. Fifty-four patients were randomized into the continuous arm and 46 to the interrupted arm. The average age of the patients in the continuous arm was 36.37 years and in the interrupted arm it was 40.09 years. Nine abdominal wound dehiscence were noted in the emergency group. Of 9 patients who developed a burst, there were 5 males and 4 females. Their average age was 34.4 years with a range of 26 to 61 years. Burst abdomen occurred in 1/46 = 2.17% in the interrupted group and in 8/54 = 14.8% in the continuous group. Risk ratio for burst was 0.15 (95% C.I.; 0.02 to1.13 ; P-value = 0.035). The prevented fraction was 85.3% (95% C.I.; 13% to 98.1%). Burst Abdomen and Anemia Out of 39 anaemic patients, 6 developed burst, whereas among 60 patients without anaemia only 3 experienced burst. The RR for burst= 1.82 (95% CI, 1.06 to 3.11; P = 0.148). Burst Abdomen and Peritonitis The relative risk for burst with peritonitis as exposure was 1.86 (95% CI; 1.36 to 2.55). The attributable fraction is 46.3% (95% C.I. ; 26.3 to 60.8% ; P-value = 0.031). Burst Abdomen And Abdominal Distension All the cases of dehiscence of the abdominal wound had abdominal distension. Burst Abdomen And Coughing A total of 65.65% had no coughing, 2.02% had atelectasis, 17.17% had chronic obstructive airway disease (COAD), 12.12% had asthma and 3.03% had bronchopneumonia. 5.88% of patients with COAD, 8.33% of patients with asthma and 33.33% of patients with bronchopneumonia developed dehiscence thus showing that postoperative bronchopneumonia could be a significant factor in predicting a high risk of burst. Burst Abdomen and Abdominal Malignancy One out of 6 cases of malignancy and 8 out of 93 without malignancy developed burst. The RR for this is 2 (95% C.I.; 0.26 to 15.3; P-value = 0.44). Burst abdomen occurred between 6th and 12th post-operative day. Logistic Regression Analysis A multivariate analysis was carried out assuming exposure to be interrupted method of suturing and outcome of interest to be dehiscence. This analysis showed that intraperitoneal sepsis, abdominal distension, coughing and anaemia were important risk factors. Multivariate Logistic Regression Final Model The log odds (ln) of burst could be computed by the following equation :- ln (Burst) = a+b1 (Method) + b2 (Sepsis) + b3 (Anemia) + b4 (Cough) Where a = - 4.0, b1 = -1.9423, b2 = 0.7141, b3 = 2.0528, b4 = 0.9616 Please see details of this analysis in Appendix 1. Result in Elective Group Of 110 patients, 56 were treated by continuous and 52 by interrupted method. Two patients in the interrupted group and none in the continuous arm experienced burst. The RR is indeterminate due to 0 in one cell. Fisher's P was 0.23. DISCUSSION Abdominal wound dehiscence remains a major cause of morbidity following any laparotomy whether elective or emergency. The burst abdomen is associated with high morbidity of up to 40% and mortality of up to 18% in elderly or malnourished patients in whom a burst represents a final additional insult to their already stressed physiology. Many randomized trials in the West have reported equal wound complication rates following the use of continuous or interrupted monofilament fascial closure.6,9-11 In our set up patients undergoing elective laparotomy have also achieved a statistically similar risk of burst in both the groups. However, our experience shows that those undergoing emergency operations with multiple factors adverse to healing, suffered from burst in 9% of cases. Indian authors have reported burst abdomen to occur in 10% to 30% of emergency cases.1,8,13 30% burst abdomen was reported in infected cases by Professor Naithani's unit from Allahabad.1 Protein calorie malnutrition is widely prevalent in the Indian population. The problem gets cmpounded with the onset of consuming diseases like tuberculosis, typhoid and cancer. Many patients undergoing emergency laparotomy suffer from one of these co-morbid conditions, detrimental to healing. Rural hospitals and nursing homes often keep patients with perforative peritonitis on conservative therapy( antibiotics and even steroids). At laparotomy we observe profound necrosis of the aponeurotic layers of abdomen in these cases. Such necrotic linea alba does not hold sutures well which cut out with a bout of coughing or sneezing. In a continuous suturing cutting out of even a single bite of tissue leads to opening of the entire wound. This is the probable explanation for a high prevalence of burst in our emergency group. There were 8 bursts in the continuous arm of suturing (dehiscence risk = 14.8%) whereas only 1 dehiscence took place (dehiscence risk = 2.17%) with the X-technique, indicating a much lower risk of burst with interrupted method of closure. This difference is clinically and statistically significant. Results indicate that our patients seem to fare better with interrupted closure techniques. Other Indian authors also report protection from burst by interrupted technique.1,8 We have performed some basic mathematical calculation on forces working across the suture line. The continuous suture is associated with a hacksaw effect due to varying tension on different parts of suture due to abdominal wall movements. This results in cutting out of the suture. In case of interrupted x-suture there is no hack-saw effect hence cut out force is minimal (Please see Appendix 2). Our data in emergency group supports this theoretical explanation. The low dehiscence in the elective laparotomy group can be explained by the fact that patients do not have any intraperitoneal sepsis, have less abdominal distension, their malnutrition and anemia are corrected prior to surgery and they are operated in a more controlled setting where errors of technique are minimal. CONCLUSIONS
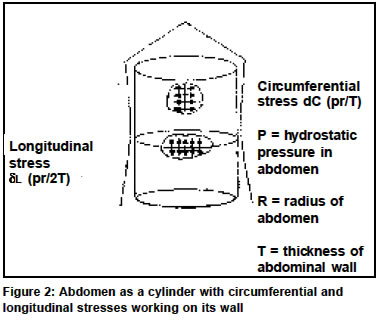
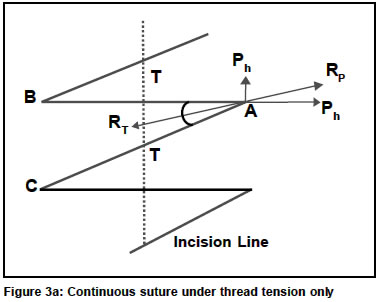
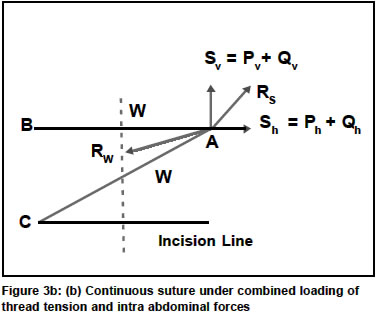
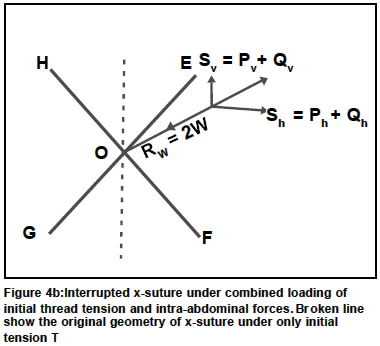
Recommendation Interrupted X-closure in presence of intraperitoneal sepsis, abdominal distention, chest infection, anaemia, malnutrition and other risk factors. Appendix 1: Detailed description of Multivariate Logistic Regression The multivariate logistic regression analysis was carried to find any association between predictors and the presence of a burst. After determining the coefficient values of interest for each model a goodness of fit test was carried out to determine how well each model fitted the observed results. A model was constructed using the logistic regression to get the following equations. (In all of these models, 0=absence of the particular risk factor and 1= presence of the risk factor). ln refers to the log odds of getting the burst abdomen in the presence of a particular variable(s). Positive coefficient values (alpha, beta) increase the risk while negative values decrease the risk. Model 1 method of suturing ln (burst) = a+b1(method) codes for method; 1= interrupted and 0= continuous . Model 2 method and intraperitoneal sepsis ln (burst) = a+b1(method) + b2 ( sepsis). Model 3 method and coughing ln (burst) = a+b1(method) + b2 (coughing) Model 4 method, sepsis and malignancy ln (burst) = a+b1 (method) + b2(sepsis) + b3 (malignancy). Model 5 method, sepsis and anaemia The equation was ln (burst) = a+b1( method) + b2 (sepsis) + b3 (anaemia). Model 6 including method, coughing and sepsis. ln (burst) = a+b1 (method) + b2 (sepsis) + b3 (coughing). Model 7 including method, coughing, sepsis and anaemia. The equation was: ln (burst) = a+b1 (method) + b2 (coughing) + b3 (sepsis) + b4 (anaemia). Model 8 included method, coughing, sepsis, anaemia and malignancy The equation was: ln (burst) = a+b1 (method) + b2 (coughing) + b3 (sepsis) + b4 (malignancy) +b5 (anaemia). To compare all the above models a G value was calculated which was -2x (log likelihood of smaller model log likelihood of larger model). This likelihood ratio test indicated that the difference between models 1 & 8 was largest and that difference between models 7 & 8 was not significant (i.e. P>0.05). This implied that dropping malignancy from the model did not make any significant difference. Presence of malnutrition completely predicted risk of burst abdomen, in that none of the well nourished patients (serum albumin>3g/dl, n=46) had burst while 9/53=16.98% cases in the malnourished group (serum albumin<3g/dl, n=53) developed a burst. Similarly, presence of abdominal distension (regardless of cause) also predicted risk of burst completely. None of the 4 patients without distension had a burst while 9/95=9.47% had a burst among patients having abdominal distension. Because of the ability of these two variables to completely predict risk of burst, the models incorporating malnutrition and distension were automatically dropped by the statistical software. The Hosmer- Lemeshow goodness of fit test was applied to choose the most appropriate model. Model 7 with anaemia, intraperitoneal sepsis and coughing had the best fit with the observed data. The model can be used to predict the risk of burst in a patient with a particular combination of risk factors. For example a patient with sepsis, anaemia and coughing who gets interrupted suturing has a chance of burst as follows: By entering the codes (see in methods section ) for method=1, coughing=1, sepsis=1 and anaemia=1 and values of a and b coefficients in the Model 7 equation below: ln (burst) = a+b1 (method) + b2 (coughing) + b3 (sepsis) +b4 (anemia), we get the following: ln (burst) = -4+(-1.9423) + 0.9616 + 2.0528 + 0.7141 = -2.2138. Therefore the odds of burst = 0.177 and probability of burst =0.15 which means a 15% chance of developing a burst. For a patient with similar risk factors treated by continuous method of suturing the odds of burst = 0.808 and probability of burst =0.45 which means a 45% chance of developing a burst. Thus interrupted method of suturing is better than continuous method in patients having multiple risk factors. Appendix 2: Mathematical considerations of stresses on abdominal wall. Continuous suture repair has some obvious shortcomings. To offset these shortcomings we have developed a new, "Interrupted X technique" for the closure of abdomen. We have attempted to explain the benefit of this interrupted suture with the principles of vectors.16-17 The sutured abdominal wall and the suture thread have to withstand two kinds of forces: One, caused due to initial tightening of the thread by the surgeon and two, the forces caused due to abdominal distension and patients movement etc. Abdominal distension caused by intestinal dilatation, collection of fluid, force of coughing etc. generates stresses in the abdominal wall. These stresses can be approximated by modelling human abdominal cavity as a cylinder with its long axis along the spine. If p is the pressure exerted by the intra-abdominal contents on the abdominal wall, the wall is subjected to longitudinal and circumferential stresses as shown in Figure 2. The two stresses are given by the following equations: Longitudinal stress (si ) = pr/2t (1 ) Circumferential stress (sc) = pr/t (2) where p = hydrostatic pressure in abdomen ; r = radius of abdomen; t = thickness of abdominal wall. It is obvious from the equations (1) and (2) that the circumferential stress at any point is double that of the longitudinal stress. Hence longitudinal midline or paramedian incision is mechanically more vulnerable than the horizontal transverse incision. However in emergency situations most surgeons prefer a midline incision because it provides better access to all the intra-abdominal organs. Integrity of abdominal wound repair depends upon tissue holding capacity of suture and suture holding capacity of tissue. Since most surgeons choose a strong thread like No. 1 Polypropylene or Polyamide (which has a high tensile strength), most wound failures are essentially a consequence of tissue breakdown (thread cutting through aponeurotic layers of abdominal wall). Assuming that the abdominal wall doesn't have any gross specific directional weakness for the cut through phenomena i.e. the thread cutting through the abdominal wall, the following analysis provides a good comparative analysis of the efficacy of the two methods of suturing namely: A. Continuous Z Method and B. Interrupted X Method. A. Continuous Z Method Figure 3a shows an example of a Continuous Z Suture commonly used by most surgeons. In this figure, T is the initial tension applied while tying the knots of the suture. It is important to highlight here that since the thread is free to slide through the abdominal wall (polypropylene or nylon are very smooth and virtually glide through the tissue), the thread tension will always be the same throughout the length of the thread. In Figure 3b, Ph and Pv are the components of the reactive abdominal wall forces caused due to thread tension T in the directions perpendicular and parallel to the incision line respectively. For equilibrium, it is necessary that the resultant Rp of Ph and Pv must be equal and opposite to the resultant RT of the tensions T in the two arms of the thread at point A as shown in the figure. Since the tensions in the arms AB and AC of the suture ought to be equal, the orientation of RT will always be in the direction bisecting the angle ÐBAC. The tension in the thread will rise with the increase in the intra-abdominal forces or patient's movement as explained above. Now, because of various factors such as non-equality of longitudinal and circumferential stresses (as highlighted through equation 1), non-homogeneity and anisotropicity of the abdominal wall, it is almost impossible that the resultant of the additional forces generated in the abdominal wall at point A by coughing, flatulence or movement etc. will be in the same direction as that of the force vector RT as highlighted in Figure 3b. Let Qh and Qv be the components of the additional forces induced at point A perpendicular and parallel to the line of incision respectively due to intra-abdominal distensions or movements (Figure 3b). To counterbalance these additional forces, the tension T in the thread will have not only to increase in magnitude but has also to reorient the direction of the resultant tension (Rw) so as to be just opposite to Rs , the resultant of Sh and Sv. This is so because it is most unlikely (as stated earlier) that the resultant of Sh and Sv will also be in the same direction as that of Rp (or Rt) in Figure 3a. Hence the resultant Rs of Sv and Sh (Figure 3b) will mostly be non-collinear to Rw. The dynamic effect of non-colinearity of Rs and Rw will be to cause imbalance between the tensions in the two limbs of the thread at point A leading to slippage of the thread at the suture point as there can't be any differential in the tension in a continuous thread. This leads to distortions in the suture geometry. Thus we find that in Z suture the dynamic changes in the intra-abdominal forces cause "to and fro" movement of the thread causing hacksaw effect on the abdominal wall, leading to distortions in the suture geometry and also leading to additional redundant forces at the suture entry points. It is this "to and fro" motion of the thread (i.e. the hacksaw effect) caused due to the dynamics of abdominal pressures and stretchings that makes the continuous sutures of any configuration vulnerable to the cut through phenomena. B Interrupted X Suture In case of interrupted X suture with a central knot as shown in Figure 4a the problem of non-collinearity of active and reactive forces gets obviated. Because of the central knot in X suture all the four arms namely OE, OF, OG and OH in Figure 4a which are always in tension, are free to rotate about the central knot O - of course subject to the overall equilibrium of the individual X suture block. This freedom of all the four suture limbs to rotate independently about O enables the suture arms to balance the net resultant of the forces on the abdominal wall due to thread tension and coughing, movement etc. without causing any state of redundancy or "to and fro" movement of the thread at suture entry point (Figure 4b). Thus the absence of any hacksaw effect in the X Suture as occurring in Z continuous suture with every spurt of intra abdominal forces makes the former more efficient and safer than the latter. Continuous closure has always been regarded to compromise the blood supply to the healing edges as compared with the interrupted technique. Therefore interrupted closure has been used to advantage in situations where blood supply is precarious e.g. colon and oesophagus. In Figure 5 the blood supply to the triangles marked "t" is cut off from all sides. This will impair wound healing and thus increase the probability of cut through. In the interrupted X technique since we do not have any horizontal or vertical cross- arms, the blood supply to the healing edge is not impaired leading to decreased probability of cut through and burst abdomen. The hacksaw effect will also occur in other types of continuous sutures (Figure 5). Acknowledgements We are grateful to Dr. K. B. Sahay, Professor of Bio-medical engineering and Dr. Sneh Anand, Prof and Head, Department of Bio-medical engineering, IIT, Delhi, For undertaking detailed analysis of the stresses working on the abdominal wall in relation to suture technique. References
© 2004 Indian Journal of Surgery. The following images related to this document are available:Photo images[is04005f4a.gif] [is04005f3a.jpg] [is04005f2.jpg] [is04005f3b.jpg] [is04005f4b.jpg] [is04005f5.jpg] [is04005f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}