 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 66, No. 1, Jan-Feb, 2004, pp. 31-35 The sphincter preserving perianal fistulectomy: A better alternative R. N. Mangual, D. N. Tudu, S. P. Pattnaik, S. S. Mohanty, K. P. Prusty Department of Surgery, M. K. C. G. Medical College & Hospital, Berhampur
- 760004, Orissa, India.
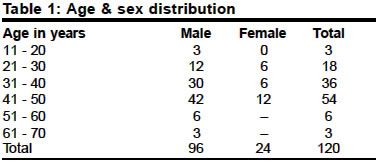
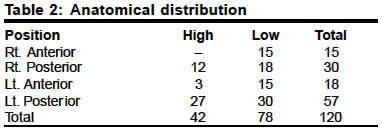
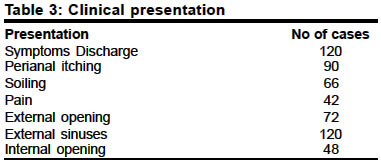
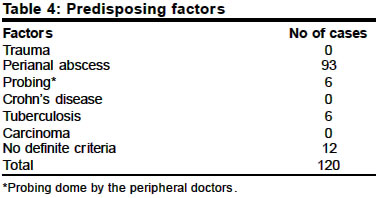
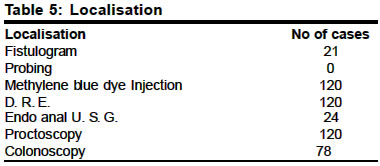
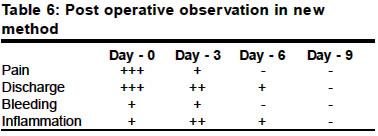
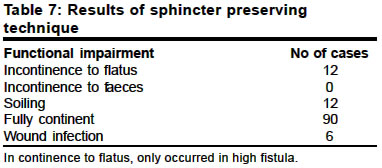
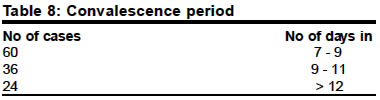
Paper Received: May 2003. Paper Accepted: October 2003. Source of Support: Nil. Code Number: is04007 ABSTRACT A fistula-in-ano is not only a common problem associated in surgical practice, but also its patho-anatomy is poorly understood by many. In this series, over a period of 12 years, 120 cases were included in the study, explained the patho-anatomy, that all the perianal fistula are not fistula, rather perianal sinus. In all the cases by a simple method of methylene blue dye injected into the tract to visualise the internal opening and condemned the probing as unscientific. The result of sphincter preserving aseptic fistulotomy, is a better alternative to conventional procedures, which avoids complications like colostomy, soiling, incontinence, morbidity and prolong hospitalisation. KEY WORDS Fistuna-in-ano, Anal fistula, Perianal sinus. How to cite this article: Mangual RN, Tudu DN, Pattnaik SP, Mohanty SS, Prusty KP. The sphincter preserving perianal fistulectomy: A better alternative. Indian J Surg 2004;66:31-5. INTRODUCTION Anal and perianal diseases, especially fistula-in-ano by their nature are embarrassing to the patient. This disease not only stresses the patient through soiling and foul smelling discharge but also causes panic. On the contrary, over enthusiastic operative treatment results in ever embarrassing faecal incontinence. Patients often complain to troublesome symptoms interfering with daily obligations. Above all, fistula-in-ano is a common surgical problem in Indian community. Majority of them develop from perianal abscesses resulting from poor personal hygiene and hot and humid climate. The perianal abscesses burst spontaneously and some of them are drained inadequately by inexperienced practitioners. When an abscess connects both perianal skin and anal canal and rectum, it is a fistula, lined by granulation tissue. But in maximum number of perianal abscesses connect only to the perianal skin, so it is a sinus not a fistula. Many surgeons have a wrong conception about the pathoanatomy of the fistula. Hence, most of the perianal sinuses are treated as fistula which complicates the scenario. Over the centuries the probing of the fistula tract as the procedure of choice and laying open a fistulous tract (fistulotomy) was the treatment of choice.1-9 This usually results in recurrence in most of the cases due to reinfection from the anal canal. Similarly the treatment of high fistulas was looked upon as a high risk job, which results in incontinence resulting from sphincter damage. The probing has become controversial and no body recommends it. The concept of performing a colostomy while treating a high fistula-in-ano, gives the patient a shocking affair, which is usually unacceptable to the patient. Lockhart Mummery has rightly pictured the surgeons mentality as "More reputation are lost in the treatment of fistula than in any other operation". This paper intends to bring a rational concept about the pathoanatomy of fistulae with their proper localisation and claims the sphincter preserving procedure with encouraging results. MATERIAL AND METHODS This study was done over a period of 12 years from January 1990 to December 2002 and total of 120 cases were included in the study. Out of which, 96 cases of males and 24 cases of females. The youngest patient was 16 years old and the oldest patient was 65 years. This study included 42 cases of high fistulae and 78 cases of low fistulae. All the cases were examined in detail with a clinical history, thorough general and local examination with baseline routine investigations. Before the fistulae were examined locally, a low cleansing enema was given for good evacuation of the tract. Then digital rectal examination (DRE) and with good illumination proctoscopy were carried out. In all the cases attempt was made to palpate the fistulous tract digitally and to feel the internal opening. Probing was never done, as it is a procedure to be condemned. Some patients were subjected to fistulogram and endoanal ultrasonography for the delineation of the tract. Methylene blue dye injected in all cases through the external opening to delineate the tract, which was a very safe and effective procedure. In most of the cases the dye did not appear in the anal canal, implying that there is no internal opening. However, in 48 cases where internal connection was there, the dye was seen coming through the internal opening. Preoperative Preparation All the patients were advised sitz bath, anti-inflammatory drugs and suitable antibiotics were given for reducing the edema and clear formation of the tract. The patients were given laxatives for two consecutive nights before operation. On the day of operation a proctcolys enema was given for cleaning the lower gut to minimise contamination. The New Procedure In the OT, the patient was given low spinal / epidural or general anaesthesia and then kept in lithotomy position. DRE and Proctoscopy were done for palpating the fistulous tract and to visualising the internal opening. Methylene blue was injected with a cannula in all cases for outlining the tract and to find out the internal opening. Then an elliptical incision was given around the perianal opening and the tissues were well dissected on either side. The lateral skin margin was retracted away from the fistulous tract by Allis forceps and the medial side was retracted with claw retractor or right angled retractor to prevent accidental opening of the anal canal. The Methylene blue dye helped in preventing the accidental injury to the fistulous tract. In the high fistulae, the sphincter muscles were carefully separated from the tract with thin bladed retractors to prevent damage to the sphincters. It is interesting to note that during dissection, at a particular point the tract was no longer present and it was abruptly missing at the terminal part of the dissection. The tract was easily separated without manipulation or difficulty. In 48 cases where internal openings were present, as evident by the methylene blue, in the anal canal. The tract was dissected in the same way till the internal opening and then the connection with the anal mucosa was obliterated with delayed absorbable suture (vicryl) from out side. In all cases the wound was obliterated by interrupted with delayed absorbable sutures. RESULTS We observed that 120 cases with fistula-in-ano under different criteria and the findings were tabulated. The condition was more prevent in the 5th decade of life and was common in males (Table 1). This study shows prevalence was 65% of the low fistulae. The fistulae were more commonly found in 87 Cases (72.5%) the posterior position out of which the left posterior quadrant 57 cases (47.5%) was mast commonly found (Table 2). All the 120 cases presented with discharging sinuses and 90 cases (75%) complained of perianal itching and soiling was noted in 66 (55%) (Table 3) cases. Proctoscopy and DRE showed internal opening in 48 cases (40%). Detailed clinical history was taken in all cases. 93 cases (77.5%) gave definite history of perianal abscess in the past and 6 (5%) cases developed fistulae as a result of probing (Table 4). In 9 cases (7.5%) multiple fistulae due to tuberculosis. We had no cases of Crohn's diseases or carcinoma in our series. Localisation was an important aspect for which all cases were subjected to proctoscopy, DRE, Methylene blue injection in to the sinus to delineate the tract (Table 5). Fistulogram was done in 21 (17.5%) cases. Endoanal USG was done in 24 cases (20%) and in no case probing was done. The cases were postoperatively observed with respect to pain, discharge, bleeding etc. on days 0, 3, 6 and 9 respectively (Table 6). As the days passed from 0 - 9, the pain discharge and bleeding became less and less. The inflammation was also subsiding within 3 days and on the 6th - 9th day there was no inflammation present in the wound. In the post operative period, 90 cases (75%) were fully continent only 12 cases (10%) complained of incontinence to flatus and wound infection was present in 6 cases (5%) only (Table 7). Majority of the cases attained convalescence within 7 - 9 days (Table 8). DISCUSSION Fistula-in-ano can result from a number of clinical conditions. Majority of the patients give positive past history of perianal abscess in our country. In fact, perianal abscesses are fairly common in the Indian community due to poor personal hygiene and hot and humid climate. Multiple fistulae can occur due to other reasons like, Crohn's disease, actinomycosis, malignancy etc. in western countries. In contrast, the Indian patients with multiple fistulae have tuberculosis as the underlying cause. We have not included multiple fistulae in the preset series for the sake of convenience and treated with antitubercular drugs. Anorectal abscesses and fistulae are commonly (45%) seen in 4th and 5th decade as in the present series. Chronic discharging sinuses in the perianal region with a past history of perianal abscess is a common observation in these cases. In the present series most of them were low type fistulae (40%) present in the lower half, peculiarly most (62.5%) fistulous tracts were present on left side. All of the patients presented with discharging sinuses and 75% perianal itching. Normally a fistula-in-ano is believed to be a tract lined by granulation tissue which connects deeply the anal canal or rectum and superficially on the skin around the anus. This usually results from an anorectal abscess which bursts spontaneously or is drained inadequately. An anorectal abscess may produce a tract, the orifice of which resembles that of a fistula, but in 60% does not communicate with the anal canal or the rectum. By definition, this is a sinus not a fistula.6 Thus all the discharging sinuses around the anal canal may be regarded as sinuses until they are proved to be fistulas. Clinically with proctoscopy and digital rectal examination (DRE), it is not possible to say whether an internal opening is present or not. Demonstration of the internal opening and delineation of the tract are important steps before surgery. The probing has been suggested by many authors to be carried out under anaesthesia, but it should never be done. Probing not only painful but creates a false passage and is converts a sinus into fistula at times. In several cases it reawakens the dormant infection in the tract. Radiography (fistulogram) is also not very rewarding. Hence, we have done fistulogram in only 21 cases (17.5%) only. Methylene blue serves as an excellent tool when injected into the tract for its delineation both preoperatively and intraoperatively. It shows internal opening, if present, as the dye escapes into the anal canal or rectum through the internal opening. Recently the use of M.R.I. and endoluminal ultra-sonogram have further facilitated the delineation of complicated and high fistulae and thus the localisation of fistula has been made easier.2,7,8 In the present series we found external opening with discharging tracts in all cases. But methylene blue showed internal openings in 48 (40%) cases only. The rest 72 (60%) cases were actually cases of sinuses resulting from inadequate drainage of perianal abscesses. Similar observations has also noted by Graf and Aeberhard and Deen, William et al. who could detect internal opening is two cases out of 18 cases in their series. The treatment of fistula has remained a challenging job for the surgeons. Since last 500 years it has been recommended by the John of Ardane to lay open the tract, from it termination to its source. This establishes a communication between the anal canal or rectum and the perianal skin this allowing constant re-infection. This may be the reason, why lot of fistulous tracts treated by fistulotomy ends up with recurrence. Thus, in this new procedure we had dissected the fistulous tracts clearly off the surrounding tissues till its origin and was excised. The wound was closed in layers. This prevented re-infection and accelerated the healing by primary intention. The treatment of high fistulas (trans-sphincteric and inter- sphincteric) has always created fear in the minds of surgeon, as it requires sphincterotomy, which results in incontinence post operatively. For this the Matod et al. at St. Marks hospital had devised a sphincter preserving approach, which had continent sphincters in 9 out of 13 cases.5 We had also treated the high fistulae in the similar fashion. In the present series only 12 cases (28.57%) had incontinence to flatus and fully continent sphincters were present in 30 cases (71.42%). Several techniques have been advocated with the aim of reducing the recurrence and complications, by various setons, endoanal advancement flaps and re-routing of tracts.4 But the theoretical advantage of this present method is, that it avoids flap mobilisation and potential hazards of ischemic necrosis and anastomotic breakdown associated with that manoeuvre. Many have recommended the treatment of high fistula under the cover of colostomy. Colostomy is a drastic procedure for this purpose and it is better to be avoided, as not accepted by patient easily. The post-operative events were highly satisfactory in the present method. The pain, bleeding, discharge had subsided by the 3rd post-operative day, and these were almost absent on 6th Post-operative day. Majority of the cases had early convalesce which was about 7-9 days. CONCLUSIONS Fistula-in-ano is common problem associated in the surgical practice, but many surgeons have poorly understood its patho-anatomy. A perianal fistula, is not a fistula always, rather it is a perianal sinus in majority of cases and probing should be condemned, as it not only painful, but convert sinus to fistulous tract. The sphincter preserving fistuloectomy, done carefully with due tissue respect, is an aseptic procedure, healed by primary intention, with not only low recurrence rate, but also avoids complications like incontinence, colostomy, soiling, injury to anal sphincter and prolong hospitalisation. So, no doubt the sphincter preserving fistulectomy is a better alternative to conventional procedure, for avoiding the complications and better result in recurrence point of view. REFERENCES
© 2004 Indian Journal of Surgery. The following images related to this document are available:Photo images[is04007t3.jpg] [is04007t2.jpg] [is04007t4.jpg] [is04007t1.jpg] [is04007t6.jpg] [is04007t5.jpg] [is04007t7.jpg] [is04007t8.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}