 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 66, No. 1, Jan-Feb, 2004, pp. 36-40 Laparoscopic approach to benign esophageal disorders K. P. Balsara, C. R. Shah, N. H. Patell, H. Shah, B. Jamaiwar, P. Gupta Laparoscopic and GI Surgical Departments, Bhatia General and Jaslok Hospitals,
Mumbai, India.
Paper Received: July 2003. Paper Accepted: October 2003. Source of Support: Nil. Code Number: is04008 ABSTRACT Background: The technique of laparoscopic surgery (LS)
has taken rapid strides over the past decade. Though the biliary tract has
been the main focus of LS, the surgical treatment of benign esophageal disease
is an area of growing interest. In this article we outline our experience using
LS in the treatment of benign esophageal diseases.
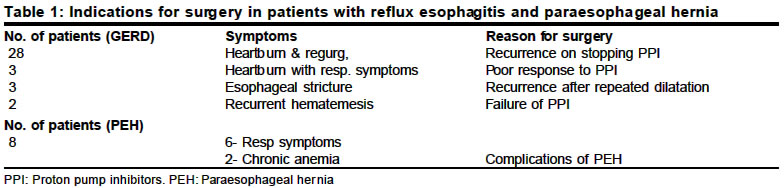
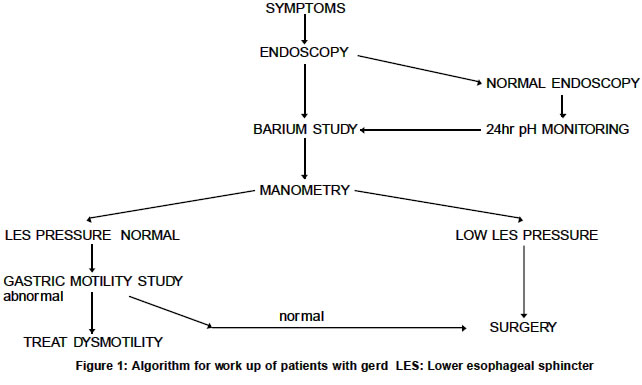
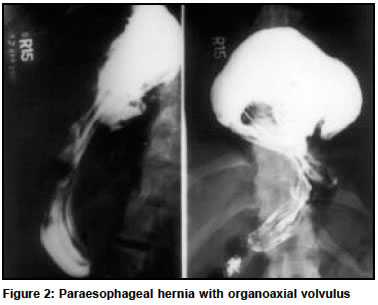
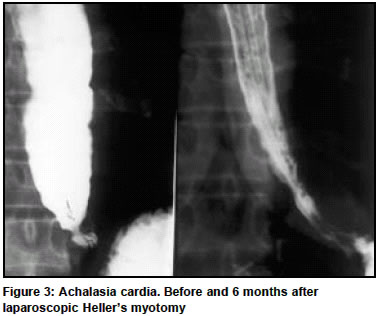
Key Words Laparoscopic surgery, Benign esophageal disease. How to cite this article: Balsara KP, Shah CR, Patell NH, Shah H, Jamaiwar B, Gupta P. Laparoscopic approach to benign esophageal disorders. Indian J Surg 2004;66:36-40. INTRODUCTION Laparoscopic surgery has gained rapid acceptance in the last decade by patients and surgeons. The biliary tract has been the main focus of LS, however, there is a rapidly growing interest in the laparoscopic approach to benign esophageal disease. In this retrospective study, we outline our experience using a laparoscopic approach in the surgical treatment of benign esophageal disorders, over a four-year period. MATERIAL AND METHODS From March 1999 to February 2003, 36 patients with GERD (27M/9F, age 7-72years), 8 with PEH (3M/5F, age 35-79 years) and 16 with achalasia cardia (6M/ 10F, age 15-65 years) have been operated upon using laparoscopic access. Patients had an upper GI endoscopy, a barium study and a routine preoperative evaluation. A manometric evaluation was done in all patients with achalasia and in the last 5 cases of GERD. The indications for surgery are shown in Tables 1 & 2. The operative technique for GERD and PEH have been detailed elsewhere.1 Briefly, under general anaesthesia and the patient in supine position 5 ports were used. One port in the epigastrium for a liver retractor (Nathanson, Cook surgical, Australia), the other 4 ports were placed in a semicircular fashion well above the umbilicus. Most of the dissection was done using a Harmonic scalpel (Ethicon surgical). The esophagus was mobilized well into the mediastinum so that about 4 to 5 centimeters of length could be brought into the abdomen. Both vagii were preserved. The short gastric vessels were always divided. The diaphragmatic crura were repaired using 1/0 prolene suture (Ethicon surgical). A loose 360-degree fundal wrap was done over a 50FG bougie using 2/0 ethibond suture (Ethicon surgical) in 35 patients; 1 patient had a 270-degree partial fundoplication. The wrap never exceeded 2 centimeters. Patients with PEH had in addition, removal of the hernial sac from the chest. In 2 patients with PEH a fundoplication was not possible due to the large volume of the sac at the cardio esophageal junction. In these patients the stomach was fixed to the abdominal wall using 2/0 silk. In patients with achalasia, the placements of ports and patient position were similar to the other cases. Only the anterior and lateral surface of the esophagus was exposed. The cardioesophageal junction was cleared of fat. The myotomy was made using a monopolar hook cautery for 5 centimeters on the esophagus and 1.5 to 2 centimeters onto the stomach. The myotomy was made to the left of the anterior vagus, occasionally the vagus had to be lifted off to preserve it. Bleeding from the edges of the myotomy was controlled using gauze pellets dipped in 1:200,000 adrenaline solution. Mucosal tears if any, were repaired with 4/0 Vicryl suture (Ethicon surgical). An anterior Dor fundoplication2 was done using 2/0 ethibond suture. Post operatively patients with achalasia had a water soluble contrast study done 24 hours after surgery to look for any leak. All patients were allowed oral liquids the day after surgery and then a soft diet for the next 3 weeks. All oral medication was stopped. Patients were followed up 1 month after surgery, then every 3rd month for the 1st year and 6 monthly thereafter. A repeat endoscopy or a barium study was done on follow up only if patients complained of heartburn or dysphagia. RESULTS The manometric findings in all patients with achalasia showed incomplete relaxation of the LES With poor motility of the esophageal body. In patients with GERD the LES pressure in all was less than 10 mm Hg (range 6 to 9 mmHg) (normal 15 to 25 mmHg). Four patients had normal Esophageal body motility but in one patient the motility was severely impaired (less than 50) (Normal more than 75 mmHg) All procedures were completed using laparoscopic access. The time taken for surgery in the GERD and PEH group was 90 to 240 minutes (mean 120) and for the achalasia patients 120 to 180 minutes (mean 140). Operative complications in the GERD group included 2 patients who developed a left sided pneumothorax, but none required chest drainage. One patient had an intrathoracic perforation of the esophagus during passage of a bougie. This occurred due to repeated passage of the bougie, which apparently would not move beyond the mid esophagus. The perforation went unnoticed during surgery and the patient was re-admitted 7 days later with a right-sided empyema, which needed intercostal drainage. An esophagogram revealed that the perforation had sealed. He subsequently made an uneventful recovery and is free of symptoms 3 years after surgery. Since this episode of perforation we have switched from using a gum elastic bougie to a mercury weighted bougie (Pilling Corp. US.) In patients with achalasia there were 2 mucosal tears. Both were sutured laparoscopically with 4/0 Vicryl. Four patients with GERD have been lost to follow up. The other 56 patients have been followed up regularly from 3 months to 4 years (mean 2.8 years) Delayed complications in the GERD group include "gas bloat" in 7; only one of these patients was distressed by this symptom for 6 months after surgery but the problem has now abated. One patient with esophageal stricture developed dysphagia 3 years after surgery and needed an endoscopic dilatation. One female patient developed severe retching and bloating 10 days after surgery, these symptoms would remain for a few days then recede. Repeated endoscopy and a barium study revealed no abnormality. A radio nuclide scan using a bread meal tagged with radiotracer (Technitium 99) showed severe gastric dysmotility (more than 50% of tracer was retained in the stomach after 4 hours) She underwent a gastro-jejunostomy 6 months after the fundoplication and her retching has stopped, but she still gets bouts of `bloating'. The other 29 patients are free of symptoms and are off all medication Delayed complications in the achalasia group include reflux in 2 patients, which can be easily controlled with short courses of proton pump inhibitors (PPI). Only one patient with a sigmoid esophagus who had several procedures before surgery complains of dysphagia 1 year after surgery. The rest of the patients have normal swallowing. DISCUSSION Gastro-esophageal reflux disease, paraesophageal hernias and achalasia cardia are eminently suited for laparoscopic surgery. In the past these patients were often denied open surgery for fear of morbidity and prolonged hospital stay. Studies have now shown that the results of laparoscopic surgery in these patients are as good as open operations with a reduced morbidity and earlier return to work.3,4 GERD is a significant problem in the West.5 In India the incidence of severe reflux is less6 but the problem continues to grow as we adopt a more westernized lifestyle. The medium to long-term results of laparoscopic fundoplication for GERD has shown a good result in over 90% of cases.7,8 The most common reason to operate on our patients was a recurrence on stopping PPi . Three patients had a poor result with PPi therapy. This could have been due to volume reflux or an associated bile reflux. Our results with laparoscopic surgery for GERD have been gratifying. Of the 36 cases operated,(18 have been reported in a previous publication.1 We have been able to follow up 32. Three patients have had a poor result, 1 due to excessive "gas bloat", 1 recurrent stricture and 1 undiagnosed gastric motility problem that needed further surgery. Twenty-nine patients (80%) have had a good result. As our experience has grown we have changed our pre operative work up in these patients to try and optimize results (Figure 1). Manometry is now done in all patients. This gives important information about the lower esophageal sphincter (LES) pressure and whether there is any esophageal dysmotility. A severe dysmotility would prompt us to do a partial fundoplication, as we have done in 1 patient. Recent literature however, suggests that the dysmotility is a result of severe reflux and these patients do best with a 360-degree fundoplication.9 Patients who have symptoms suggestive of reflux but normal LES pressures, could have an underlying gastric motility problem and this should be ruled out by a radionuclide scan before surgery. (Figure 1). One of our patients had a gastric dysmotility and fundoplication made her symptoms worse. She had to undergo a gastrojejunostomy for relief. Paraesophageal hernias are uncommon, occur in older patients and almost always require surgery, due to a high rate of complication,10 (Figure 2). They are more difficult to treat than patients with GERD, but with experience the results improve.11 Our results with PEH have been encouraging and all 8 patients remain symptom free in the medium term. In spite of most of these patients not having reflux symptoms, most authors recommend an antireflux procedure in addition to repair of the diaphragmatic crus since reflux can occur in up to 65% of these patients in the post operative period.12 Achalasia cardia is the commonest primary motility disorder of the esophagus, characterized by a hypertensive LES and poor esophageal body motility.13 Historically achalasia was always treated surgically either by a trans-abdominal or trans-thoracic route. With the advent of endoscopic pneumatic dilatation there was a paradigm shift in management of these patients and pneumatic dilatation became the first line treatment, with surgery being resorted to when repeated dilatation failed. Botulinum toxin injection into the LES, a more recent introduction, gained only temporary acceptance as the results were too short lived. Only one prospective randomized controlled trial comparing open surgical myotomy and pneumatic dilatation has shown that surgery had superior results in the long term.14 Recent reviews comparing the outcomes of different treatment modalities showed surgical myotomy as the most effective form of therapy.15,16 With the ability to do a Heller's myotomy through laparoscopic access with results as good as open surgery and without its attendant morbidity, should now tilt the scales in favour of LS. Our own experience with achalasia, albeit a small one, has been satisfactory (Figure 3). Of the 16 patients treated 13 had previous dilatations ranging from 2 to 4 in number. Two patients had botox injections in addition to dilatation and a further two had surgical myotomy which had failed. (Table 2) In spite of these previous procedures 15 out of 16 patients have had a good result with laparoscopic myotomy on follow up ranging from 3 months to 3 years. The single patient with a poor result is a 50-year-old male who had undergone an open trans-thoracic Heller's, 2 dilatations and one botox injection. He has a mega esophagus and is a candidate for esophagectomy. Previous dilatation and botox injection makes the myotomy difficult and a higher incidence of perforation has been reported.17,18 Both perforations in our series occurred in patients with previous botox therapy. A fundoplication added to the myotomy serves two purposes, a) it keeps the edges of the myotomy apart and b) prevents reflux. Our preference is to do an anterior Dor fundoplication without dividing the short gastric vessels, rather than a posterior partial wrap. This prevents damaging tissue behind the esophagus, which may have a role in the antireflux mechanism. CONCLUSIONS Laparoscopy gives excellent access to the cardioesophageal junction and is eminently suited for the surgical treatment of benign esophageal disease. Patients with GERD need careful selection and a proper work up for optimizing results. PEH is more difficult to treat surgically than GERD, but as experience increases the results are as good as open surgery. We believe laparoscopic myotomy for achalasia should be the treatment of choice, especially in younger patients who are fit for surgery. Pneumatic dilatation and botox injection should be reserved as therapy for those who have recurrent symptoms after a myotomy or in older patients unfit for surgery. REFERENCES
© 2004 Indian Journal of Surgery. The following images related to this document are available:Photo images[is04008t1.jpg] [is04008f1.jpg] [is04008f2.jpg] [is04008t2.jpg] [is04008f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}