 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
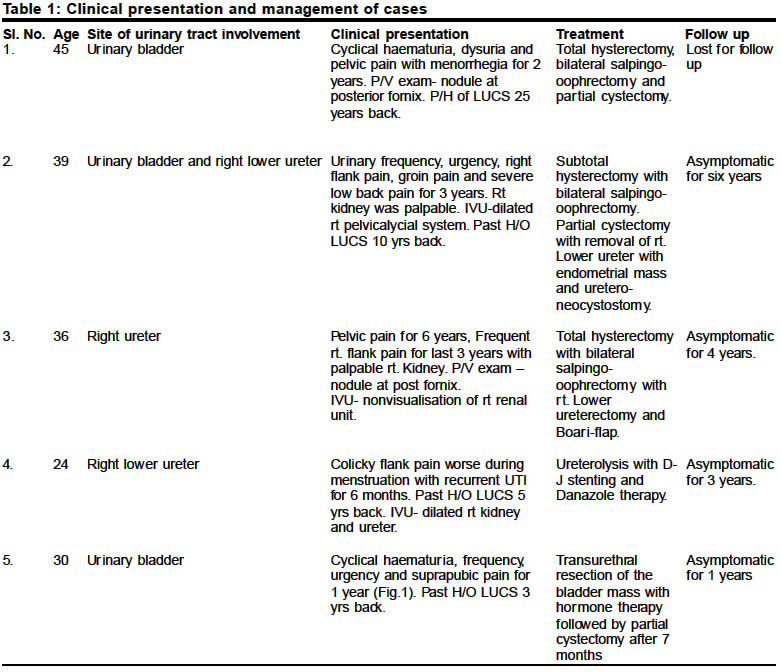
Indian Journal of Surgery, Vol. 66, No. 1, Jan-Feb, 2004, pp. 41-43 Urinary tract endometriosis Dilip Kumar Pal Department of UrologyBankura Sammilani Medical College, Bankura, West Bengal
- 722102, India.
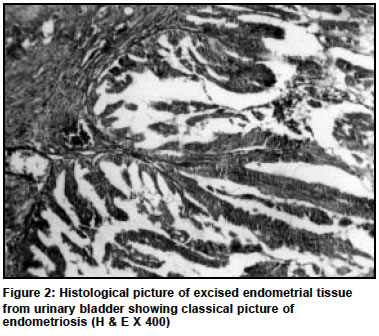
Paper Received: April 2003. Paper Accepted: May 2003. Source of Support: Nil. Code Number: is04009 ABSTRACT Endometriosis is a common problem in women of childbearing age with multifocal sites of involvement in the pelvis. But urinary tract involvement with endometrial tissue is rarely seen. Here we report our experience of five patients with urinary tract endometriosis with their outcome. Key Words Endometriosis, ureter, urinary baldder, ultrasonography. How to cite this article: Pal DK. Urinary tract endometriosis. Indian J Surg 2004;66:41-3. INTRODUCTION Endometriosis is defined as the presence of ectopic endometrial tissue outside the normal confines of the uterine cavity. These ectopic lesions may consist of endometrial glands and/or stroma and may interfere with normal physiological process by their infiltrative nature or by the formation of adhesions. Endometriosis was first described by Russel in 1955.1 Abeshouse and Abeshouse(1960) on an extensive collective review on urinary tract endometriosis found 127 cases of vesical, 15 ureteral, 6 renal and pararenal and 3 urethral endometriosis.2 Ureteric involvement first described by Cullen(1917) in a patient with bilateral ureteric involvement.2,3 Since then 98 cases of ureteric endometriosis have been reported in English literature and 5 in Japanese literature; eight of them had bilateral involvement.3 Here we describe our experience of five cases of urinary tract endometriosis of which two had vesical and three had ureteric involvement. MATERIALS AND METHODS This study was undertaken at Urology Department of Bankura Sammilani Medical College and Hospital, Bankura for a period of seven years from 1996 to 2002. All the cases were referred from Gynaecology OPD. Among the five patients one was retrospective (Case No.1) and the others were prospective cases operated by the author. All the patients were examined thoroughly with special emphasis to pervaginal examination. Investigations like haemogram, blood sugar, renal biochemical parameters, USG of renal tract and lower abdomen were done in every patient. Intravenous urography was done in patients with loin pain or dilated pelvi-calycial system on USG. Diagnostic laparoscopy was done before operation to assess the surrounding organ involvement by endometriosis. Cystoscopy was done in all patients to note any vesical endometriotic nodule and retrograde pylography was tried in patients where renal or lower ureteric shadows were not seen on IVU. All the patients were operated and nature of operation is noted in Table 1. Follow up was done for a period of 1 year to 6 years with USG, cystoscopy or IVU. RESULTS Youngest patient of our series was of 24 years age who had a caesarian section at her 20 years of age and the oldest patient was of 45 years. Pelvic pain and low backache were present in every patient. Urinary urgency, frequency and dysuria were the outstanding symptoms. Cyclical haematuria was most commonly seen with vasical involvement. Dull aching pain in the loin was present where ureter was involved. Among five patients three had past history of caesarian section. Pervaginal examination showed nodule was on posterior fornix in two cases. Kidney was palpable in two cases. USG of pelvis and abdomen showed bulky uterus and grossly dilated upper urinary tract in three cases. On USG vesical nodule was seen in case no. 5 simulating the bladder tumour. In two cases IVU demonstrated a dilated ureter and pelvi-calycial system and in another there was nonvisualisation of kidney. Retrograde ureterography was tried in those two cases but the ureteric catheter could not be negotiated beyond 2 cm of ureteric orifice. All the cases were operated and the nature of operation has been summarised in Table 1. The case no. 5 was operated by transurethral resection of the bladder mass with a provisional diagnosis of transitional cell carcinoma but histological diagnosis was endometriosis. Again it recurred within three months and a partial cystectomy of the tumour bearing area cured the patient. DISCUSSION Although endometriosis is a benign condition but it may have an aggressive clinical behaviour. It occurs in 15-20% women of childbearing age. Most commonly it affects the organs like ovaries, uterosacral ligaments, fallopian tubes, rectum and cervico-vaginal region.1-3 The incidence of urinary tract involvement, though uncommon is estimated to be about 1%2,3 of which vesical involvement is the most common of them.2,4,5 Usually the women of the 3rd or 4th decade of age are affected with a peak incidence in between 30-35 years.4 Chronic pelvic pain with urinary urgency, frequency, dysuria, dysparenuea with or without cyclical haematuria are the outstanding clinical symptoms. Ureteric involvement may present with backpressure changes in the kidney or anuria with bilateral ureteric involvement.3 Diagnosis of such cases are difficult due to nonspecific symptoms. High index of suspician to all symptomatic women with a history of caesarian delivary or other gynaecological surgery gives a clue to the diagnosis. USG is the initial step of investigation to detect the vasical endoluminal mass or upper urinary tract dilatation.IVU is still very much useful to detect the integrity of the upper tract and ureter. Cystoscopy and biopsy may give a clue to the diagnosis before operation. Retrograde ureterography may show the length of ureteric involvement. Abdominal laparoscopy is useful to assess the extensiveness of the disease. MRI or CT scan does not provide any different or precise information than an ultrasound scan.6 Treatment varies according to the severity and site of involvement of each case. Hormonal therapy with danazole does have a definite roll in regressing the lesion but in cases with urinary tract involvement, surgical treatment is a better option because the condition may lead to kidney loss up to 25%.3 Aggressive surgical treatment with removal of ectopic tissue, relief of urinary obstruction and castration with or without hysterectomy is recommended following a reasonable parity if there is urinary tract involvement.3 In the younger patients with reproductive capability endometriosis should be resected with or without hormonal treatment and urinary function should be reviewed with preservation of ovarian function with strict periodic surveillance of urinary tract integrity.2,3 In the present series all the cases were managed by open surgery and the nature of the surgery done is summarised in table no.1. But nowadays the pendulum has swung more in favor of laparoscopic surgery.7-9 Ureteric involvement is nowadays being managed by laparoscopic ureterolysis with excision of endometrial tissue and laparoscopic partial resection of the ureter with uretero-ureterostomy or neo-cystostomy.9 Even transurethral resection of vesical endometriosis may be a valid therapeutic option in selected cases,10 but in our case the disease recurred again within three months after transurethral resection. So such cases with endoscopes management check cystoscopy is strictly advised. REFERENCES
© 2004 Indian Journal of Surgery. The following images related to this document are available:Photo images[is04009t1.jpg] [is04009f2.jpg] [is04009f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}