 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 66, No. 1, Jan-Feb, 2004, pp. 46-47 Case Report Unusual sites of mycetoma G. Mallikarjuna Rao, K. Devanandam, M. Janaki,* K. Lakshmireddy** Departments of surgery, *Pathology & **K. L. R. Pathology Lab, Kurnool
General Hospital, Kurnool - 518002, India.
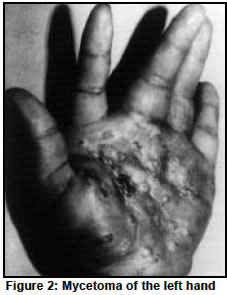
Paper Received: January 2002. Paper Accepted: February 2002. Source of Support: Nil. Code Number: is04011 ABSTRACT Mycetoma is a localised, chronic, progressive and granulomatous inflammatory lesion caused by certain fungi or bacteria. It is characterized by gradually increasing painless tumour like swelling with appearance of multiple sinuses, discharging pus and granules .We report 3 cases of unusual sites of Madura Mycetoma, affecting the chest, hand and knee .All the cases were treated by surgery followed by antifungal drug Fluconazole postoperatively.The causative species isolated being Madurella Mycetomatis in histological sections. No recurrences were observed. KEY WORDS Madura Mycetoma, Sinuses, Madurella Mycetomatis. How to cite this article: Rao GM, Devanandam K, Janaki M, Lakshmireddy K. Unusualsites of mycetoma. Indian J Surg 2004;66:46-7. INTRODUCTION Mycetoma exists in many tropical and subtropical countries between latitude of 150 south and 300 north. It is widely prevalent in India. Endemicity of disease in South India is well established. How ever, cases have also been reported from other parts of this country. The common sites of Mycetoma Mycetoma being foot, hand, perineum, head and scalp. Sometimes rare sites like eyelid, testis, lymphnodes, middle ear cleft etc are involved. CASE REPORTS Case 1 A 25-year-old man presented with discharging sinuses from the right upper chest since 1 year. No history of pyrexia, cough and dysnoea. Past History suggestive of carrying dried maize splintrs on the chest and shoulders is present. Radiography of the chest revealed normal bony cage and lungs. On excision biopsy of the sinuses(5 sinuses) showed, the features of Mycetoma caused by Madurella Mycetomatis. The post operative follow up for 6 months showed no recurrence. Case 2 A 55-year-old man presented with a nodular swelling over the lateral side of the right knee since 10 months. The nodules showing discharging sinuses since 2 months. No history of pyrexia, pain and difficulty in walking. Past history of trauma with iron nail was present 1½ year back (Figure 1). Radiography of the right knee showed no bony abnormality. On excision biopsy, features of Mycetoma caused by Madurella Mycetomatis. The postoperative followup for 1 year showed no recurrence. Case 3 A 35-year-old women presented with a swelling of left hand with multiple discharging sinuses since 2 years. No history of trauma and pyrexia .The patient is a agricultural field worker. The movements of the wrist and fingers are restricted (Figure 2). Radiography of the left hand showed massive osteolytic lesions of the carpels, metacarpels and phalanges was noted. The biopsy of the lesion showed features of mycetoma caused by Madurella Mycetomatis. Hence below elbow amputation of the left forearm was done followed by histopathological confirmation of the specimen for Mycetoma. The post operative follow up for 6 months showed no recurrence. All the above 3 cases had Fluconazole 50 mg per day for 3 months postoperatively. DISCUSSION Mycetoma was first recognised as a clinical entity in Madurai (South India) as madhura foot, but now it is known to be prevalent in other countries also. Foot continues to be the commonest site followed by the upper extremity.1 Involment of the perineum as the third in order of frequency and the fourth commonest site was scalp. The aetiological factors involved in causation are multiple in the form of thorn prick, trauma leading to ulceration, blunt trauma and the wicks. The clinical picture of Mycetoma is almost uniform irrespective of the causative fungi.2 Histology of Mycetoma has achieved a reasonably good standard in identification of species, that more sophisticated tests are not desired as a routine as they very cumbersome and time consuming and it is evident that Madurella Mycetomi is the prevalent fungus.3 Radiological examination was done in suspected cases of bone involement. The radical cure can be achieved by local excision followed by antifungal therapy for 3-6 months and by amputation of the affected part, in case the bones were affected.4 REFERENCES
© 2004 Indian Journal of Surgery. The following images related to this document are available:Photo images[is04011f2.jpg] [is04011f1.jpg] |
| |||||||||

{kind=link}
{kind=link}