 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 66, No. 1, Jan-Feb, 2004, pp. 47-49 Case Report A rare presentation of primary hydatid cyst Samir M. Kacheriwala, Ketan D. Mehta, Biju Pillai, Yogesh Jain Department of surgery, M. P. Shah Medical College, G. G. Hospital, Jamnagar
- 361008, India.
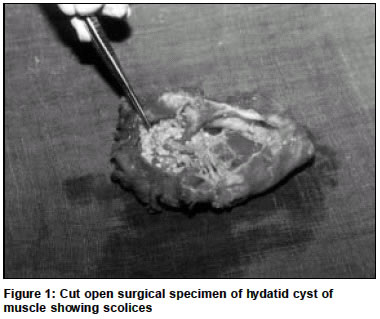
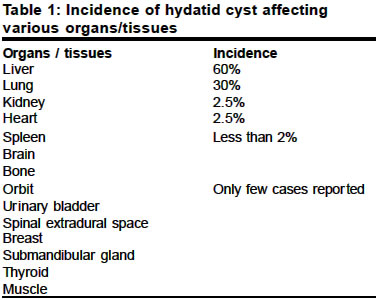
Paper Received: September 2002. Paper Accepted: January 2003. Source of Support: Nil. Code Number: is04012 ABSTRACT Hydatid cyst affecting a muscle is very rare. The clinical diagnosis of which requires high index of suspicious. The diagnosis can be made by careful history, physical examination and simple investigation like ultrasonography and fine needle aspiration. Surgical excision of cyst remains the mainstay of management. Key Words Hydatid cyst, Muscle, Echinococcus granulosus. How to cite this article: Kacheriwala SM, Mehta KD, Pillai B, Jain Y. A rare presentation of primary hydatid cyst. Indian J Surg 2004;66:47-9. INTRODUCTION Hydatid disease is endemic in developing countries and cattle rearing regions of the world.1 It may affect wide range of organ or tissue. Here we present a case of hydatid cyst of muscle which according to contemporary literature is a relatively rare occurrence. CASE REPORT A 20-year-old female from the family of shepherds was admitted with a painless swelling over left side of back since 3 months. There was no history of trauma, fever or weight loss. Physical examination revealed a diffuse, non-tender cystic swelling of 20 x 12 cm in size over the left infra scapular region with fixity to deep muscles. On blood examination the Total Leukocyte Count was 5000 cells ul-1 and 1% eosinophils. Routine chest radiograph and abdominal ultrasound was normal. A plain radiograph showed a large soft tissue mass in infra scapular region of left back with normal underlying bones. Ultrasound of local part show cystic lesion with some echogenic material inside it. Fine needle aspiration from the cyst was performed to differentiate hydatid cyst from cold abscess, which yielded clear fluid and microscopic examination of fluid was inconclusive. Based on these findings, a working diagnosis of hydatid cyst arising from muscle was made. On exploration, a hydatid cyst deep to lattisimus dorsi muscle and attached to serratus posterior inferior muscle was found. The cyst was excised and soft tissue washed with 0.5% cetrimide solution. When the specimen of cyst cut opened, multiple scolices were found inside it (Figure 1). Histopathology confirmed our working diagnosis of hydatid cyst. Post operatively the patient was put on medical treatment in form of Tablet Albendazole 400 mg daily and follow up of the patient till today is uneventful. DISCUSSION Hydatid disease is caused by the larval tapeworm of the genus Echinococcus granulosus, Echinococcus multilocularis and Echinococcus oligarthrus. Echinococcus granulosus is the most common cause of hydatid disease.1The incidence1,2 of involvement of various organs and tissues by hydatid disease in descending order is mentioned in Table 1. Hydatid disease of muscle is rare. Classically the patient presents with a long history of cystic lump with muscle fixation. Routine investigations like complete blood count, x-rays and ultrasonography of abdomen and local part should be carried out first. Aspiration of fluid by fine needle is safe,3 simple and effective means to reach working diagnosis. Serological tests like ELISA and immunoelectrophoresis are important tool in diagnostic workup if diagnostic dilemma persists, provided facility of such tests is available. However all of these may not be conclusive. Hydatid cyst is classically confirmed by direct demonstration of parasitic elements in surgical specimen.1 The treatment of hydatid cyst is principally surgical. However pre-operative medical treatment should be considered in order to sterilize the cyst, to decrease the tension in the cyst and thus reducing the chances of spillage and resultant anaphylaxis. Intra operatively, the instillation of 0.5% cetrimide, 15% hypertonic saline or 0.5% silver nitrate solution before opening the cavity tends to kill the daughter cysts and thus prevents further spread and anaphylactic reaction. Post operative medical treatment reduces recurrence rate.4 REFERENCES
© 2004 Indian Journal of Surgery. The following images related to this document are available:Photo images[is04012f1.jpg] [is04012t1.jpg] |
| |||||||||

{kind=link}
{kind=link}