 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 66, No. 1, Jan-Feb, 2004, pp. 49-50 Case Report Delayed dehiscence of repaired urinary bladder Puneet Dargan, Bhupendra K. Jain Department of Surgery, BP Koirala Institute of Health Sciences, Dharan, Nepal.
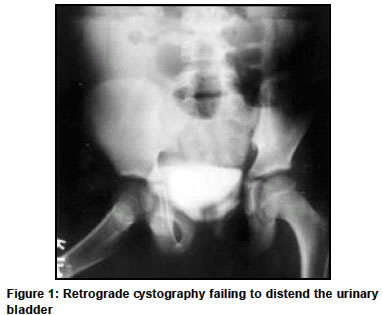
Paper Received: August 2002. Paper Accepted: December 2002. Source of Support: Nil. Code Number: is04013 ABSTRACT Delayed dehiscence of a previously repaired bladder rupture in a 12-year-old boy is described. There was no obvious cause except that while in bed the boy had withheld his early morning urge to pass urine. He presented with peritonitis and raised urea and creatinine levels. Retrograde cystography was diagnostic after the urinary catheter had drained 1.2 litres of blood-tinged urine. The rent in the dome of the bladder at the site of previous repair was closed with polyglycolic acid sutures during emergency laparatomy. Though rarely reported, delayed dehiscence is a possibility which can occur in repaired urinary bladder. It emphasizes the need for long-term follow-up. KEY WORDS Bladder rupture, Delayed dehiscence, Spontaneous. How to cite this article: Dargan P, Jain BK. Delayed dehiscence of repaired urinary bladder. Indian J Surg 2004;66:49-50. INTRODUCTION Idiopathic spontaneous urinary bladder rupture is a rare entity. It is neither associated with bladder disease nor with any outlet obstruction.1 Idiopathic delayed spontaneous dehiscence of a previously repaired bladder rupture, though known, has been reported once in the literature.2 We hereby report a case of delayed idiopathic dehiscence of repaired bladder rupture in a child and postulate possible aetiologies. CASE REPORT A 12-year-old boy was hospitalized with a history of generalized abdominal pain of sudden onset and abdominal distension of 24 hours duration. He had no history of fever, vomiting, or constipation, but he had passed very little urine since the onset of pain. Following blunt abdominal trauma 36 months ago, he had undergone an exploratory laparotomy. A splenorrhaphy, primary repair of an ileal perforation and repair of an intraperitoneally ruptured bladder were performed. He had recovered uneventfully following surgery and had maintained good health without any urinary complaints. On examination, the child was alert and afebrile. He had tachycardia and his respiratory rate was 20/min. Abdomen showed a midline scar and was distended. He had tenderness and guarding all over his abdomen. Shifting dullness was present. Laboratory examination revealed an essentially normal blood count, but his blood urea was elevated to 92 mg/dl and serum creatinine was 5.0 mg/dl. Serum sodium and potassium were 130 meq/l and 5.8 meq/l respectively. Plain X-ray abdomen and chest were within normal limits. Emergency ultrasonography showed intraperitoneal fluid collection. A Foley catheter was placed to monitor the urine output. It immediately drained about 1.2 litres of blood-tinged urine. The patient's abdominal distension subsided with the drainage of urine. The possibility of intraperitoneal rupture of bladder was entertained and immediately a retrograde cystography was performed. It failed to distend the urinary bladder despite instillation of 400 ml. of contrast, suggesting a bladder perforation (Figure 1). The patient underwent abdominal exploration which revealed a 2 cm-long rent at the site of the previous scar on the dome of the urinary bladder. The rest of the bladder was normal and there was no evidence of backpressure changes inside the bladder. The rent was repaired in two layers with polyglycolic acid sutures. He recovered uneventfully and was discharged with normal urea and creatinine levels. DISCUSSION Spontaneous rupture of urinary bladder is rare. In most patients an underlying pathology is implicated. In a smaller minority the rupture is idiopathic.1 Idiopathic rupture of a previously repaired bladder can be regarded as delayed dehiscence of the repaired bladder.2 In this patient no immediate aetiology could be elicited except that the boy had postponed his early morning urge of micturition while in bed. Clinical features of bladder rupture are remote and non-specific.3,4 A high index of suspicion is required to diagnose a bladder rupture.5 Following catheterization, sudden relief of pain and distension, or draining small amounts of infected or blood-stained urine raises the possibility of bladder rupture.6 A retrograde cystogram should always be performed immediately, which along with voiding cystourethrography is regarded as an investigation of choice.4,7,8 The delay in presentation and diagnosis results in significant reabsorption of urea and creatinine through peritoneal dialysis and manifests as raised urea and creatinine levels.4,7,8 Ascitic fluid creatinine: Serum creatinine ratio > 1.0 is suggestive of an intraperitoneal urine leak.7 Raised serum levels of ammonia and potassium have also been reported in cases with urinary ascites.5 Re-exploration and repair of the bladder, preferably in two layers after trimming the edges has shown better results.5,8 Non-operative management is also advocated, but it is reported to have a higher chance of recurrent spontaneous rupture.9 Following repair of the bladder for rupture, spontaneous or traumatic, the patients should be educated, regarding bladder emptying, to prevent over-distension. Urodynamic studies should also be done,1 to exclude any outflow obstruction in patients of spontaneous rupture. The delayed dehiscence in this patient highlights the need for postoperative follow-up. However, the rarity of the clinical situation does not allow exact standards of follow-up to be defined. REFERENCES
© 2004 Indian Journal of Surgery. The following images related to this document are available:Photo images[is04013f1.jpg] |
| |||||||||

{kind=link}