 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 66, No. 1, Jan-Feb, 2004, pp. 51-52 Case Report Hepatic metastases of a gastrointestinal stromal tumour Sharada R. Rane, Izhar N. Bagwan, Vasudeo V. Holla, Mukund M. Joshi* Departments of Pathology and *Surgery, B. J. Medical College & Sassoon
Gen. Hospitals, Pune, India.
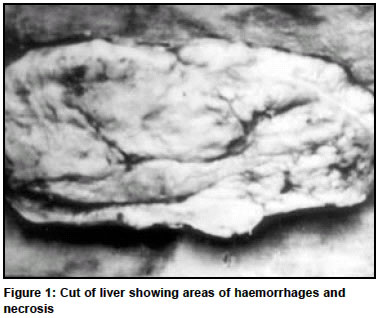
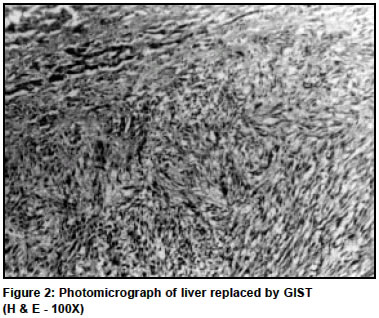
Paper Received: June 2002. Paper Accepted: October 2002. Source of Support: Nil. Code Number: is04014 ABSTRACT Gastrointestinal stromal tumours are rare visceral neoplasms. Some 3% to 38% of them have malignant histological features and are associated with a high incidence of recurrence. We present a patient with liver metastases from a malignant GIST. Key Words Gastrointestinal stromal tumour, Metastasis. How to cite this article: Rane SR, Bagwan IN, Holla VV, Joshi MM. Hepatic metastases of a gastrointesyinal stromal tumour. Indian J Surg 2004;66:51-2. INTRODUCTION Gastrointestinal stromal tumours constitute the largest category of primary nonepithelial neoplasms of stomach and small bowel.1 The precise cellular origin of GIST has been proposed to be the interstitial cell of Cajal, an intestinal pacemaker cell which on ultrastructural examination has characteristics of both smooth muscle and neural differentiation.2 In recent years these tumours have become a subject of controversy as 3% to 38% of them have malignant histological features and that metastases occur in upto 68% of these patients. Gastric stromal tumour (autonomic neural type) forms one of the components of Carney's triad (which also includes pulmonary chondroma and extra-adrenal paragangliomas).3 CASE REPORT A 50-year-old male presented with complaints of a painful, gradually increasing lump in the abdomen of 3 months duration. He also had experienced a dull ache in the epigastrium which was intermittent and not associated with intake of food, nor relieved by any medications. He had previously undergone resection of a jejunal mass which was shown to be a GIST. Abdominal examination revealed a mobile, non-tender, firm mass measuring aproximately 12 x 10 cm in the left hypochondriac and epigastric region. The mass was clinically indistiguishable from the liver. Scar of previous surgery was seen on the abdomen. Per rectal examination was normal. Hematological and biochemical investigations were within normal limits. Ultrasonography and CT scan of the abdomen revealed a 11.5 cm x 10 cm mass occupying the left lobe of the liver. Subsequently laparotomy was done followed by a left hepatic resection for removal of the tumour en mass which weighed approximately 3½ kg. The post-operative recovery was uneventful. On gross examination, the liver mass was 20x15x10cm in size. The cut surface was yellowish, fish flesh like with areas of haemorrhages and necrosis showing a rim of normal compressed liver tissue at one end (Figure 1). Histopathology revealed a tumour comprising of spindle shaped cells arranged in fascicles, pallisades, and whorls with minimal nuclear pleomorphism and occasional mitotic figures (Figure 2). On immunohistochemistry, the tumour cells were strongly positive for S100, vimentin and weakly positive for smooth muscle actin. The final diagnosis reached was of gastrointestinal autonomic nerve tumour (GANT). DISCUSSION Patients with GIST are predominantly of middle or elderly age group.3 As in our patient, the most common clinical presentation is pain with lump in abdomen. It should be kept in mind that the percentage of malignant cases is higher in GIST of small bowel than in those for the stomach.1 Recurrence of GIST is usual and one report found only 10% of patients to be free of disease after long-term follow up.3 The most common site of metastases of malignant GISTs are the liver, peritoneum and lungs. Although, these metastases usually take as long as 30 years to develop after removal of the primary tumour1, in our case metastasis to liver occurred within a short period of 3 years. In recent years it has been found that most of the GISTs are positive for CD117 (C-kit protein) and therefore considered by some as the defining feature of GIST.4 Further, stromal tumours with smooth muscle differentiation are strongly positive for smooth muscle action whereas the gastrointestinal autonomic nerve tumours are positive for S100 and vimentin.1,4 In our case, the tumour cells were strongly positive for S100 and vimentin. Thus, immunohistochemistry is mandatory for further subtyping and for determining the malignant potential as these tumours may look absolutely benign on morphology. The treatment of GIST is primarily surgical. The high rate of local and distant recurrence warrants the need for adjuvant therapy. Radiation therapy is of limited value.3 Systemic chemotherapy in the form of KIT Tyrosine Kinase inhibitor drug STI-571 (Gleevac; Novartis, Basel, Switzerland). has been proposed for treatment of metastatic GIST.5 REFERENCES
© 2004 Indian Journal of Surgery. The following images related to this document are available:Photo images[is04014f2.jpg] [is04014f1.jpg] |
| |||||||||

{kind=link}
{kind=link}