 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 66, No. 2, Mar-Apr, 2004, pp. 78-83 Post mastectomy immediate breast reconstruction experience in a high volume centre in India Irshad Ahammed A. Shaikh, Harun Thomas, Ramesh Vidyadharan, V. S. Pushpangadhan, Santhosh John Abraham Department of Surgery, Lourdes Hospital, Cochin - 682012, India.
Paper Received: September 2003. Paper Accepted: November 2003. Source of Support: Nil. Code Number: is04019 ABSTRACT Early diagnosis and multi-modality treatment for carcinoma breast has resulted in the prolonged survival of many patients with carcinoma of breast. It is important that the surgeons who handle breast malignancies look at the psychological and cosmetic aspects without compromising the oncological principles of surgery in carcinoma of the breast. Post-mastectomy immediate breast reconstruction (IBR) addresses the psychological and cosmetic problems that follow mastectomy. There are various techniques available for post mastectomy primary breast reconstruction. An ideal technique should be affordable to the majority of economically poor patients and should be less time-consuming. During the period of seven years from January 1996 to December 2002, we operated 2032 cases of carcinoma breast, of which 346 patients had IBR using various procedures. In our centre, TRAM flap was found to be the best procedure for post-mastectomy IBR. Whenever possible, immediate reconstruction is the best. Presence of the tissue used for reconstruction was not found to affect any form of local adjuvant treatment like radiotherapy, or delay the detection of local recurrent disease. Key Words Carcinoma breast, Mastectomy, Immediate breast reconstruction, Transverse rectus abdominis myocutaneous flap (TRAM flap). How to cite this article: Shaikh IAA, Thomas H, Vidyadharan R, Pushpangadhan VS, Abraham SJ. Post mastectomy immediate breast reconstruction experience in a high volume centre in India. Indian J Surg 2004;66:78-83. INTRODUCTION During the Halstedian era, which lasted many years, radical mastectomy was the treatment offered for carcinoma breast. In fact, Halsted warned against closure of the breast wound after the surgery.1 Hence attempts to reconstruct breast after mastectomy had to wait for many years. Today the concepts have changed and it is more of Breast Conservative Surgery. This has been made possible because of early detection, better investigative facilities, increased understanding of the pattern of disease spread and better forms of adjuvant treatment options. Despite the condemnation of the reconstruction of breast, Vincent Czerny tried it for the first time in 1895 by transplanting a large lipoma of the flank to the mastectomy site, and it was reported that the patient was doing well after one year.2 Tansini described the use of the latissimus dorsii myocutaneous flap for the first time in 1906 for a breast reconstruction.3 In 1942 Sir Harold Gillies described pedicled flap from abdomen with multiple stages for reconstructing breast.4 It was Manchot's landmark work on vascular territories of the body that ignited the interest of many, to develop different types of flaps, including axial flaps.5 A good number of patients do come in the early stages of the disease due to improved awareness and the availability of better diagnostic tools. Better survival and improved quality of life have increased the expectations of these patients as well of the surgeons. Fortunately, today's woman need not live her life with an anatomical deficiency and a cosmetic problem, which adversely affects her psychology and her social movements. Breast reconstructions, and mainly immediate breast reconstructions,6 have come to help these women who have undergone mastectomies. Compared to delayed reconstruction, IBR reduces the total hospital expense and total period of hospital stay.7 In India, the percentage of patients who can be offered a conservative breast surgery for a malignant breast disease has not attained a sizeable proportion. We still do get patients presenting in the late stages of the disease, requiring only toilet mastectomies. Forty per cent patients, diagnosed to have breast cancer, still undergo mastectomy because of multifocal pathology, non-conservable disease status as suggested by inappropriate breast / tumour size ratio, or by choice of the patient.8 Many of these women can be offered primary reconstruction and a good majority accepts this mode of therapy. The most common method of breast reconstruction is a Transverse Rectus Abdominis Myocutaneous (TRAM) flap because of its texture and large volume.9 Other flaps used to reconstruct the breast are LD flap, inferior gluteal flap, superior gluteal flap, etc.10 MATERIAL AND METHODS Lourdes Hospital, Cochin, Kerala, India is a 750-bedded general hospital working at a tertiary referral level. The General Surgical department performs about 2500 major operations and about 3500 minor operations every year and has a predominant interest in oncology. All patients treated for carcinoma breast from January 1996 to December 2002 (seven-year period) have been included in this study. A) Whenever a patient presented to the department directly with symptoms pertaining to breast, a thorough clinical examination was done and if suspected to have a malignancy the clinical stage was noted. a) The majority of the patients presented with a lump in the breast. These patients were sent for Fine Needle Aspiration Cytology (FNAC) study.
b) If the patients with breast symptoms did not have a palpable disease a mammogram and/or a ductogram were done, depending on the symptoms along with a breast ultrasound examination to detect any mass lesion and targeted cytology / biopsy was done. B) The referred patients with a proven breast malignancy were clinically reviewed and their slides were reviewed by our pathologists/ cytopathologists and the diagnosis was reconfirmed. Once the diagnosis is established and the staging work-up is completed on an outpatient basis, the patients are offered treatment depending on their stage of the disease as per the protocol pertaining to UICC 1999 staging for carcinoma breast.11 The criteria to offer breast reconstruction are A) Stage of the disease
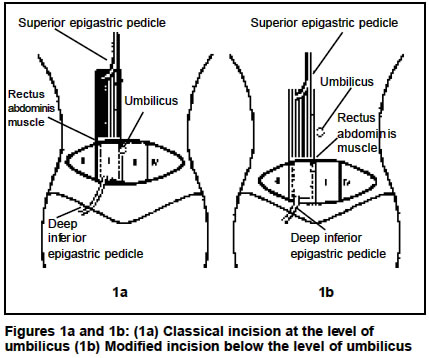
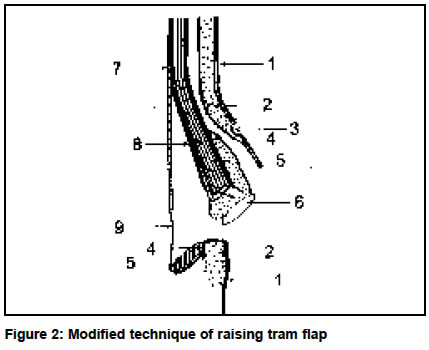
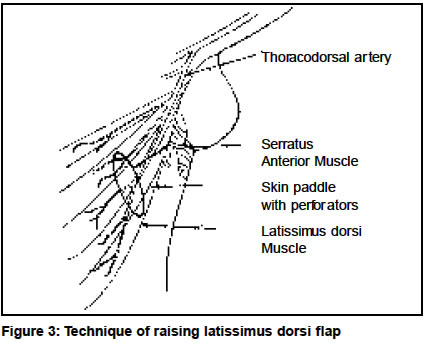
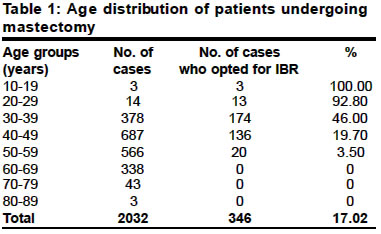
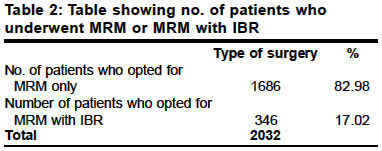
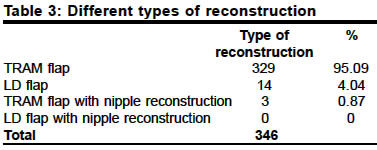
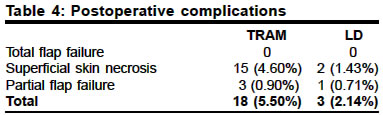
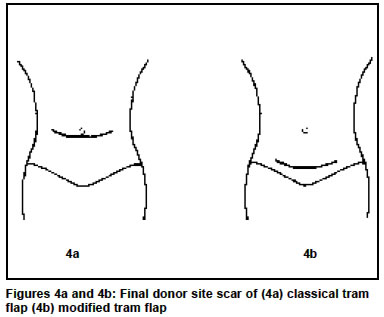
B) Likely anatomical deficiency after mastectomy: This pertained to a large group of patients who had a good-sized breast, which if removed would have certainly left behind an unacceptable anatomical deficiency. A small group of ladies with very small-sized breast having malignancy were not offered breast reconstruction as this would not have caused any significant benefit to the appearance of the lady. C) Age of the patient: Breast reconstruction was suggested only to people below the age of 60 years and also after considering their active social / sexual life. D) Mental make-up of the patient: The age, social status, educational and economic background along with the stage of the disease influences the mental attitude of the patients with breast malignancy. Breast reconstruction was offered only to those who had a very positive frame of mind and only to those who could be brought to that state after adequate counselling. E) Economic status of the patient: As the expense of the treatment would have to be borne by the patients, except in a small minority who were supported by the insurance companies, a major deciding factor in offering reconstruction to these patients, was their economic status. In our department, an added expense of Rs. 5000/- to Rs. 6000/- would have to be borne by the patients opting for a breast reconstruction. F) Educational background of the patient: Breast reconstruction was offered only to those who had clearly understood the philosophy behind this, the message of adherence to the protocol of treatment and the need for constant follow-up.12 G) Demand of the patient: Irrespective of all the factors mentioned, the patient's demand would also be taken into consideration at the time of total planning of the treatment. The surgery for carcinoma breast, in the group of patients who had primary post-mastectomy breast reconstruction, was a Modified Radical Mastectomy (MRM) (Auschinclos) where clearance of axilla is done up to Level III lymph nodes. All throughout the surgery, no sutures are used and haemostasis is achieved by bipolar cautery. The incision over the breast includes the nipple areolar complex and the skin over the tumour and it is through this incision that the breast tissue and the axilla are cleared to give the best cosmesis to the patient. If the nipple areolar complex can be spared without oncological compromise it is done to achieve a better cosmetic result. Post-mastectomy primary breast reconstruction is done with a pedicled Transverse Rectus Abdominis Myocutaneous (TRAM) flap or Latissimus Dorsii (LD) flap. Technique of raising TRAM flap Depending on the volume of tissue needed to match the other breast, the TRAM flap can be transferred on a single pedicle or a pedicle with supercharging of the flap using the cut end of the pedicle, or as a free flap. In our series, we used a single-pedicled flap, usually based on the contra-lateral superior epigastric artery.13 We used a modified technique to harvest the TRAM flap. The skin incision was made much below the level of umbilicus where the classical incision is put, so that the final scar is much more acceptable than that in the classical incision (Figure 1). The area of skin taken depended on the area needed to be covered over the mastectomy site. The skin was cut along with subcutaneous fat, obliquely, so as to include a large amount of fat of the anterior abdominal wall to provide the bulk for reconstruction. The take of fat on to the flap is up to the level of the umbilicus ensuring better vascularity with the peri-umbilical perforators retained in the flap. At the upper part of the flap the incision is extended down to the anterior rectus sheath at the level above the umbilicus. As shown in Figure 2, a plane was then created anterior to the anterior rectus sheath all the way up to the mastectomy site crossing the midline and it was through this space that the flap was taken from the donor site to the recipient area. At the lower part of the flap, the incision was extended in depth through the anterior rectus sheath to include the rectus muscle and the preperitoneal fat, where the inferior epigastric artery lies, which is divided and the upper part, the vascular pedicle of the flap, is taken along with the flap. The flap is elevated by dissecting in the plane between the rectus muscle and the posterior rectus sheath by cutting at the junction of the anterior and posterior sheaths of the rectus muscle. Thus the flap will have about 120-150 degrees of turn at the pedicle level when it is taken to the recipient area. Since the defect of the donor site is below the level of the arcus semilunaris, a polypropylene mesh is always used to create strength for the abdominal wall, thereby preventing the development of hernia. Technique of raising LD flap Incision is made depending on the area of skin needed for the cover (Figure 3). The slantingly placed vertical incision, along the posterior axillary fold, is deepened first to identify the muscle and then the skin flaps are raised to find the anterior border of the latissimus dorsii muscle which is raised off the lateral chest wall. The island of skin already marked along with the underlying tissues including the muscle is harvested to be placed in the recipient area of the mastectomy site. Reconstruction of nipple areolar complex There are different techniques for reconstructing the nipple areolar complex like tattooing, free graft using labia minora, etc. We have reconstructed only three cases of nipple areolar complex. Postoperative care Drains are placed in the area of the mastectomy site, axilla and in the area from where the flaps are taken and are removed, depending on the drainage, between the 4th to 6th postoperative day. Sutures are removed on the 7th or 8th postoperative day and the patient was discharged. Adjuvant treatment The decision regarding adjuvant treatment, like chemotherapy, radiotherapy and hormonal manipulations, is taken based on the age, size of the tumour, nodal status, menopausal status and the final histopathology report which gives an idea about the grade of the tumour and many other prognostic indices. Follow-up Regular follow-up is done once a month for the first year after finishing the adjuvant treatment, once in two months during the second year, once in three months in the third year and then once every six months. These regular follow-ups consist of a thorough clinical examination. Yearly surveillance with chest X-ray, abdominal ultrasound and mammogram of the opposite breast is done. RESULTS In the seven-year period from January 1996 to December 2002, we operated on 2032 cases of carcinoma breast, of which 346 (17.01%) patients had primary reconstruction using different procedures (Tables 1 and 2). Breast reconstruction was done using mainly TRAM flap, and LD flap was used infrequently. Nipple areola reconstruction was done in only 3 cases. We used the TRAM flap to reconstruct breast in 329 (95.08%) patients and the LD flap in 14 (4.04%) patients. Nipple reconstruction over the TRAM flap was done in 3 (0.87%) patients (Table 3). We never had total flap failure. But superficial skin necrosis and partial flap failure were seen in 18 (5.50%) patients with TRAM flap and in 3 (2.14%) patients with LD flap (Table 4). DISCUSSION Post-mastectomy IBR has definite advantages over mastectomy alone by providing good cosmesis, thereby imparting psychological benefits to the woman. The appreciation of oncological safety has lead to immediate reconstruction of breast in a single anaesthesia over the past few years. Skin-sparing mastectomy and further sparing of the nipple areola complex has improved the final appearance. Between TRAM and LD flaps, aesthetically, the TRAM flap is better, as it provides better bulk of tissues and also helps to achieve a reasonable abdominoplasty in most women. The main disadvantage of LD flap is that it provides only a limited volume of tissues and hence requires the concomitant use of a breast implant to achieve a volume match with the opposite breast. This is expensive in our economic setting. Hence we use the LD flap for breast reconstructions in very limited situations. As stated by many authors, we too observed that preserving the infra-mammary fold offers a definite advantage in IBR towards achieving a better cosmesis. The overall hospital stay of our patients was about 7-8 days and it is comparable with other authors.14 We had about 18 (5.5%) flap-related complications in the TRAM flap group, which is comparable with other studies.15 Among donor site complications we had occasional seromas but never had abdominal hernias or weakness. This may be due to the routine use of mesh for abdominal closures. Both flaps never hindered adjuvant local radiotherapy if indicated or detection of local recurrence to any extent. Initially, we used to harvest TRAM flaps at the level of the umbilicus. Currently, we harvest the skin of the TRAM flap from much lower down nearer to the wound which is to be closed with an attempt to have a more acceptable scar (Figure 4). CONCLUSION
REFERENCES
© 2004 Indian Journal of Surgery. The following images related to this document are available:Photo images[is04019t2.jpg] [is04019t1.jpg] [is04019t4.jpg] [is04019f3.jpg] [is04019t3.jpg] [is04019f4.jpg] [is04019f1.jpg] [is04019f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}