 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 66, No. 2, Mar-Apr, 2004, pp. 84-88 Polymerase chain reaction (PCR): Its comparison with conventional techniques for diagnosis of extra-pulmonary tubercular diseases R. C. Kesarwani, Anjana Pandey,* Ashutosh Misra,** Anupam Kumar Singh** Department of Surgery, M. L. N. Medical College, and associated S. R. N. Hospital,
Allahabad, India; *Centre for Biotechnology, University of Allahabad, India;
**Postgraduate student of MS (Surgery).
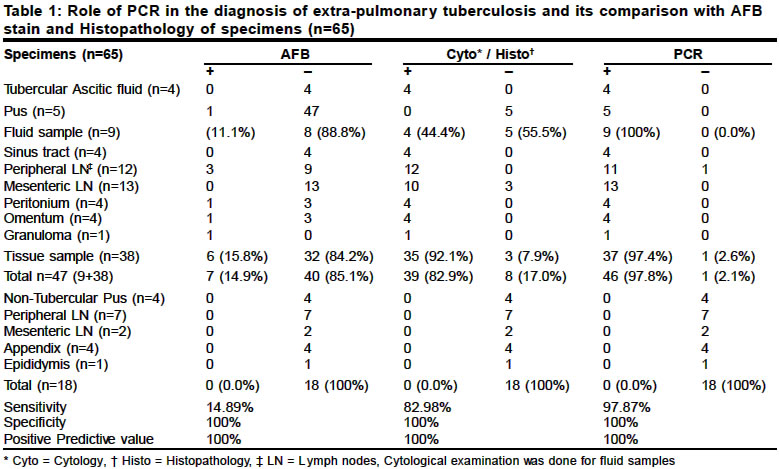
Paper Received: October 2003. Paper Accepted: December 2003. Source of Support: Nil. Code Number: is04020 ABSTRACT 65 clinical samples, which included 5 pus, 4 ascitic fluid and 38 specimens of different tissues, from 57 patients with clinical suspicion of extra-pulmonary tuberculosis were studied for AFB staining, culture for M. tuberculosis, histopathology and PCR. The study was aimed at the detection of M. tuberculosis DNA with the help of PCR in extra-pulmonary tubercular disease in its earliest stage and to compare its efficacy with other conventional diagnostic techniques. On comparing, in 9 fluid samples, only 11.1% were AFB positive, 33.3% were culture positive, 44.4% were cytologically positive and 100% were positive by PCR. In 38 samples from different tissues, 15.8% were AFB stain positive, 92.1% were histologically positive and 97.36% were PCR positive. The overall sensitivity, specificity, positive predictive value and negative predictive value of PCR were 97.87%, 100%, 100%, and 94.73% respectively. It was concluded that maximum sensitivity and specificity can be achieved by the combined use of clinical diagnosis, histopathology and PCR. PCR has a potentially important role in improving the diagnostic accuracy of extra-pulmonary tuberculosis. Key Words Extra pulmonary tuberculosis, AFB stain, culture for M.Tuberculosis, histopathology, Polymerase chain reaction. How to cite this article: Kesarwani RC, Pandey A, Misra A, Singh AK. Polymerase chain reaction (PCR): Its comparison with conventional techniques for diagnosis of extra-pulmonary tubercular diseases. Indian J Surg 2004;66:84-8. INTRODUCTION Tuberculosis is a rampant disease in developing countries such as India where the prevalence is reported to be as high as 30% of the population. Laboratory diagnosis of tuberculosis is based on the traditional methods of Ziehl Neelsen acid-fast stain and on laboratory culture of the causative organism. M. tuberculosis. The Ziehl Neelsen stain, although rapid and inexpensive, lacks sensitivity in clinical specimens. The laboratory culture of M. tuberculosis requires a long culture period and therefore, clinical and therapeutic decisions have to be made before the laboratory diagnosis becomes available. The amplification of specific DNA sequences by polymerase chain reaction (PCR) is a novel tool for the detection of mycobacterial DNA sequences in clinical specimens such as body fluids and tissues.1-2 PCR has several advantages over culture, including confirmation of the presence of M. tuberculosis within 1 to 3 days as compared to 6 weeks with conventional culture techniques. DNA amplification can be used for tissue specimens which are already formalin-fixed and paraffin-embedded.3 Many a times tissue biopsy is sent directly for histopathological unsuspecting tuberculosis until the report of microscopic examination comes to be in favour of tuberculosis. In those cases PCR amplification can be used to detect M. tuberculosis in tissue samples even though the tissues have been preserved in formalin or other substances that preclude the possibility of culture. In developing countries tuberculosis of the lymph node is the most common form of extra-pulmonary tuberculosis. In these cases a rapid, sensitive and specific diagnosis is needed, owing to the limitations of the traditional microbiological methods, paucibacillary nature of the specimen and the extensive differential diagnosis.4 Abdominal tuberculosis usually presents as intestinal obstruction or as tabes mesenterica or as tubercular peritonitis. In these cases the rapidity of diagnosis is the key for successful management, and the PCR of tissue specimen for M. tuberculosis will help in rapid and sensitive diagnosis. MATERIAL AND METHODS 65 clinical samples, which included 5 pus, 4 ascitic fluid and 38 specimens of different tissues, from 57 patients with clinical suspicion of extra-pulmonary tuberculosis were included in our study. The study was conducted in the Postgraduate Department of Surgery, M.L.N. Medical College and associated S.R.N. Hospital, Allahabad. The PCR of the specimens was done at the Centre for Biotechnology, University of Allahabad. The laboratory diagnosis of tuberculosis was made if either fluid, pus or tissues revealed AFB on Ziehl-Neelson staining, and / or grew M. tuberculosis on culture, and / or revealed tubercular granulomas with or without caseation necrosis on histological or cytological examination, and / or were positive for PCR. Those in the non-tubercular group with 18 clinical specimens were negative for tuberculosis on the basis of histopathological examination, AFB stain, culture for M. tuberculosis or PCR. All the tissue samples were divided into three portions. Two portions were fixed in 10% formalin, embedded in paraffin wax, sectioned, and each was subjected to histopathological examination and AFB staining. The third portion was suspended in normal saline and stored in a sterile container at 200C for PCR. Fluid samples were also divided into three portions, one sent for cytological examination and AFB staining, the second for culture and the third part was stored at 200C for PCR. Culture was done on Lowenstein-Jensen media. DNA extraction and purification Liquid samples These were incubated with equal volume of 4% NaOH of at 370C for 60 min with intermittent vortexing. Samples were centrifuged at 10 000 g at 40C for 15 min and the pellet was suspended in 1 ml TE (10:1) (pH 8.0). A 200 µl sample was taken in a 1.5-ml eppendorf tube and boiled for 10 min followed by the addition of proteinase K (25 µg/ml) and 200µl Lysis buffer [10 m mol Tris HCl (pH 8), 0.1 molar EDTA (pH 8), 20 µg/ml RNase, and 0.5% SDS (sodium dodecyl sulphate)]. The sample was incubated at 560C for 2 hours with intermittent shaking, then boiled at 1000C for 10 min followed by extraction with equal volume of phenol: chloroform. Aqueous supernatant was extracted once with chloroformisoamyl alcohol (24:1). The aqueous phase was taken in fresh eppendorf tube and DNA was precipitated by adding 1/10th volume of sodium acetate and 0.6 volume isopropranalol or double volume of chilled dehydrated ethanol, and was incubated for 30 min at 150C, centrifuged at 10 000 g at 40C for 30 min, and the pellet was washed twice with 70% ethanol. The DNA pellet was dried and suspended in 10 µl of 10: 1 TE. PCR The primer pairs used for the amplification of IS 6110 were CCT-GCG-AGC-GTA-GGC-GTC-GG and CTC-GTC-.CAG-CGC-CGC-TTC-GG. The PCR mixture was prepared in 50 µl of templet DNA, Deoxynucleoside triphosphate (200 µ M). Assay buffer (1.5 mM MgCl2), 0.5 µM primers (forward and reverse) and 0.5 unit Taq DNA polymerase. The reaction cycle was carried out 40 times in a DNA thermal cyclier (Perkin Elmer 2400, USA). Each cycle consisted of denaturation at 940C for 30 s, annealing at 600C for 30 s, elongation at 720C for 30 s followed by elongation at 720C for 7 min at the end of the reaction. The amplified mixture was analysed by agarose gel electrophorisis [2% agarose in Tris-Acetate EDTA buffer (pH 8)]. Tissue sample The tissue sample was washed 3-4 times in 50:50 TE pH 8. The tissue was cut into thin slices, homogenized (glass homogeniser) in 400 µl TE 10:1 pH 8 and equal volume of 10% NaOH was added and incubated at 500C for three hours with intermittent vortexing. Samples were centrifuged at 10 000 at 40C for 15 min and washed thrice with sterile distilled water. The pellet obtained was suspended in 200 µl TE 10:1 pH 8 and boiled for 10 min. Proteinase K 25 µg/ml and 200 µl lysis buffer was added and the sample incubated at 560C for 2 hours. Nucleic acids were extracted by adding equal volume of phenol: chloroform. The rest of the extraction was the same as for the liquid sample. Formalin-fixed wax-embedded tissue sample Seven 6µm thick sections were cut from each tissue block with new disposable microtome blade and the sections were treated with xylene 3 to 4 times till wax was completely removed. The tissue was rinsed once with dehydrated ethanol followed by rinsing in TE 50: 50. The rest of the procedure was the same as for the tissue sample. PCR analysis Tissues were determined to be PCR-positive when the 123-bp M. Tuberculosis DNA fragment was present on gel, and were declared PCR- negative when this fragment was absent. RESULTS This blind study included 65 clinical specimens of 57 patients to compare the different diagnostic modalities for the detection of tuberculosis and to evaluate the usefulness of PCR. The ages of the patients included in our study ranged from 5 years to 80 years with the maximum number of patients being less than 50 years of age (91.2%), with a male to female ratio of 1.4: 1; 87% patients were of low socio-economic status. The patients were divided into two groups according to the final diagnosis as tubercular or non-tubercular. The tubercular group consisted of 41 patients with 47 clinical specimens including ascitic fluid, pus, pheripheral lymph nodes, sinus tracts, mesenteric lymph nodes, peritoneum, omentum, granulomas. The non-tubercular group had 16 patients with 18 clinical specimens including specimens of pus, peripheral lymph nodes, mesenteric lymph nodes, intestinal tissue, epididymis. The final diagnosis of tuberculosis was based on clinical suspicion, AFB staining, culture for M. tuberculosis, histopathological results and PCR. AFB staining of the specimens diagnosed 7 (14.89%) out of 47 specimens with the final diagnosis of tuberculosis. AFB stain was positive in 1 (11.11 %) out of 9 of the fluid specimens and in 6 (15.79%) out of the 38 tissue specimens. All the 6 tissue specimens in which AFB was positive showed caseating granulomas on histopathological examination and all were positive on PCR. AFB was negative in all 18 non-tubercular cases (Table 1). Culture for M. tuberculosis was done only on liquid or semi-liquid specimens, i.e. 4 specimens of ascitic fluid and 5 specimens of pus from psoas abscess. Culture was positive for M. tuberculosis in 3 (33.3%) out of the 9 specimens. None of the ascitic fluid specimens was culture-positive. Three of the 5 specimens from psoas abscess were positive for culture. All culture-positive specimens were also positive for PCR and none of them could be differentiated as tubercular on cytological examination. The cytological examination of the fluid samples showed all the 4 samples of ascitic fluid in favour of tuberculosis. All the 5 samples of psoas abscess could not be differentiated on the basis of cytological examination. In the tubercular group 35 (92.10%) of the 38 tissue samples were histopathologically positive for tuberculosis. In the non-tubercular group all the 18 cases were histologically negative for tuberculosis. Of the 35 histologically tubercular-positive samples only one was PCR-negative, the rest were all positive (Table 1). In three patients the histopathological examination of the mesenteric lymph nodes was negative but the PCR of the specimen was positive for tuberculosis. One of the above patients presented with intestinal obstruction for the 2nd time within 45 days with no history of any previous surgery or abdominal tap. Laparotomy findings were thin film-like adhesions with enlarged ileal mesenteric lymph nodes. The histopathological report of the lymph nodes was chronic inflammatory but PCR proved to be positive in favour of tuberculosis and the patient responded to the anti-tubercular treatment (Table 1). The two other patients presented as acute appendicitis with mesenteric lymphadenitis. The histopathological examination of the excised mesenteric lymph nodes and appendicectomy specimens was separately reported as chronic inflammatory in both the patients. The condition of the patient did not improve even two weeks after surgery. The PCR of the wax-embedded specimens was done which was positive for the mesenteric lymph nodes of both the patients and negative for appendix specimens. Both the patients were then given anti-tubercular treatment. Patients responded to anti-tubercular treatment with a follow-up period of 6 months and 9 months each. Of the 47 specimens finally diagnosed to be tubercular, PCR was positive in 46 (97.8%) of them. All the 9 tubercular fluid samples were positive by PCR. Of the 38 tissue samples diagnosed to be tubercular, 37 (97.36%) were positive by PCR. On comparing, in fluid samples, only 1 (11.11 %) was AFB-positive, 3 (33.3%) were culture-positive, and only 4 (44.4%) were cytologically suggestive of tuberculosis while all were positive by PCR. PCR had 100% sensitivity and specificity in fluid samples. In tissue samples 6 (15.8%) were AFB-positive, 35 (92.1%) were histologically positive, 37 (97.36%) were PCR-positive. One specimen of cervical lymph node which was positive on histopathological examination was negative on PCR. A repeat PCR of this sample was done using two-fold larger aliquot of the stored specimen and though the result was still negative, the patient responded to anti-tubercular treatment. PCR had a sensitivity and specificity of 97.36% and 100% respectively on tissue samples. The overall sensitivity, specificity, positive predictive value and negative predictive value of PCR was 97.87%, 100%, 100%, and 94.73% respectively (Table 1). DISCUSSION The application of PCR to the diagnosis of extra-pulmonary tuberculosis has the potential to resolve one of the foremost challenges faced by a clinician and a diagnostic laboratory. In our study an in-house PCR test was compared with histopathology, AFB staining and culture for the detection of M.tuberculosis in 65 different specimens. In our study PCR was based on the amplification of the IS6110 insertion sequence, which belongs to the IS3 family and is found in almost all members of the M. tuberculosis complex. Most strains of M. tuberculosis carry 1015 copies, which are present in a wide variety of chromosomal sites.5-6 A study compared two PCR assays in lymph node tissue sections and concluded that the primers that targeted the IS6110 element had higher sensitivity (89%) than those amplifying the 65 Kda antigen coding gene (6%), highlighting the value of using multiple copy target.7 However there are reports that some isolates of M. tuberculosis from south India lack this element.8 AFB positivity in smears and histological specimens depends on the bacillary load of the specimen and the type of the material.9 Different studies have reported a wide range of AFB positivity ranging from as low as 0% to as high as 75%.10 In our study AFB smear of tissue samples was positive only in about 16% of the cases and all of them showed caseating granulomas on histopathological examination. Culture for M. tuberculosis was done only in liquid samples, pus and ascitic fluid; here the cytological diagnosis does not give direct evidence of tuberculosis but may be suggestive of tuberculosis. In our study the sensitivity of culture was low, about 33%. Perhaps the use of a more sensitive microbiological technique, such as liquid culture system, would result in a higher culture positivity.11 However, due to lack of these equipment in our laboratory this could not be investigated in our study. In our study there were three tissue samples in which the histological diagnosis came out to be negative and which were identified by PCR as positive on formalin-fixed, paraffin-embedded tissue, and later responded to the anti-tubercular therapy. Perhaps these are the cases where PCR can play a role in the diagnosis of tuberculosis at an early stage of the disease when conventional methods fail. These cases might represent a transition between the incubation period and the development of the disease not diagnosed by histopathology or AFB staining during the evolution of the disease in the lymph nodes. In our study there was no false positive result using PCR. Other studies in which a few false positive cases have been reported suggest a possible contamination during sample collection. There was one false negative case which even on repeat PCR with two-fold larger aliquot remained negative. False negative can theoretically be ascribed either to sampling errors, to the paucibacillary nature of the specimen, inefficient extraction of the DNA, or to the presence of PCR inhibitors. The presence of PCR inhibitors has been reported in pus samples, tissue biopsies and sputum.12 In our experience, a combination of histopathology and PCR must be applied for the rapid and early diagnosis of tuberculosis in paucibacillary specimens, especially granulomatous lymphadenopathy without necrosis or caseation. PCR might be particularly useful for the diagnosis of tuberculosis in clinical specimens where the tissue biopsy is directly sent for histopathological examination because tuberculosis was not a clinical consideration and the report comes to be in favour of tuberculosis. In those cases PCR can detect M. tuberculosis DNA even in formalin-fixed paraffin-embedded tissue as seen in two cases of our study. CONCLUSION PCR, in principle, is a highly sensitive technique that detects DNA from a single to a few micro-organisms with overall sensitivity, specificity and positive predictive value of 97.87%, 100%, and 100% respectively. AFB staining alone has positivity of only 15% and histology alone has positivity of 82.97%. The combined use of clinical diagnosis, histopathological diagnosis and PCR has a sensitivity and specificity of 100%, and 100% respectively. PCR has a potentially important role in improving the diagnostic accuracy in clinical specimens from extra-pulmonary tuberculosis seen in surgical practice. REFERENCES
© 2004 Indian Journal of Surgery. The following images related to this document are available:Photo images[is04020t1.jpg] |
| |||||||||

{kind=link}