 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
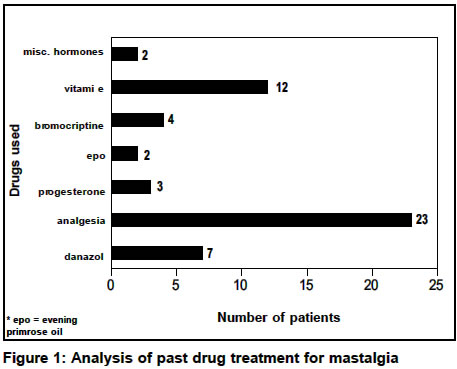
Indian Journal of Surgery, Vol. 66, No. 2, Mar-Apr, 2004, pp. 89-92 Refractory mastalgia or inadequately treated mastalgia? Krishnaswamy Uma Department of General Surgery, Apollo Hospitals, Chennai, India. Paper Received: October 2003. Paper Accepted: January 2004. Source of Support: Nil. Code Number: is04021 ABSTRACT Background: Though mastalgia is a common problem standard
algorithms of management are not always followed by clinicians. Inadequately
treated mastalgia arises as a consequence. This is labelled as refractory mastalgia
and referred to breast clinics for further treatment.
Key Words Refractory mastalgia, Inadequately treated mastalgia, Standard algorithms of Mastalgia management. How to cite this article: Uma K. Refractory mastalgia or inadequately treated mastalgia? Indian J Surg 2004;66:89-92. INTRODUCTION Mastalgia is common in both primary care and surgical outpatient settings in India.1-3 But standard algorithms of management are not universally adhered to by clinicians. This is true of India as elsewhere in the world.4 Inadequacy of treatment results in instances of mastalgia being labelled as "refractory" to treatment with referral to breast clinics for specialised management. Delayed treatment results in unnecessary physical, emotional and financial strain on the patients. This is unacceptable in itself and particularly in the context of mastalgia which is a common benign breast disorder responding, in the majority of instances, to reassurance.5 MATERIAL AND METHODS A prospective observational study was undertaken in an outpatient breast clinic setting. Fifty-eight patients, referred to the author as instances of refractory mastalgia between 2001 and 2002 were enrolled to determine whether they were true instances of refractory mastalgia or whether they were merely instances of inadequately treated mastalgia. This was done by observing their response to a protocol of non-pharmacological management. All patients were evaluated to determine the type of mastalgia, its duration, severity, past treatment and response. Further evaluation consisted of clinical breast examination, haemogram, thyroid, prolactin and lipid profile assessment. Investigations such as mammogram, fine needle aspiration cytology (FNAC), etc. were undertaken only as required. All patients were taught breast self-examination during the period of evaluation. Treatment was initiated after assessment, by reassurance, advice on a low-fat, methyl xanthine restricted diet and dietary supplementation with 500 mg/day of evening primrose oil capsules for the duration of the study (six months). Literate patients or a family member in the case of sub-literate patients were taught to maintain a pain diary during the follow-up period. The first review was undertaken three months later and the second, six months later. A simple visual analogue scale (using the individual patient as her own control) was used to quantify pain at initial assessment, and response to treatment during the two reviews. The response was graded as Grade 1 (excellent), Grade 2 (substantial), Grade 3 (poor) and Grade 4 (no response). During review, compliance with breast self-examination and evening primrose oil supplementation were noted specifically. Compliance with dietary changes of fat and methyl xanthine restriction was not assessed objectively, but was merely reiterated as a health message. RESULTS Out of 58 urban Indian women enrolled into the study, five patients were lost to follow-up. Forty-two (79.2%) patients were from Tamil Nadu and the rest from the other states: Assam (three patients), Bihar (three patients), Kerala (one patient), Meghalaya (one patient), and West Bengal (five patients). Thirty (56.6%) patients had cyclical mastalgia and 23 (43.4%) had true non-cyclical mastalgia, of a severe degree. The median duration of cyclical mastalgia was three years (mean 3.93 years) and that of non-cyclical mastalgia was one year (mean 2.35 years). The median age of cyclical mastalgia patients was 36.5 years (mean 36.63 years) and that of non-cyclical mastalgia patients was 39 years (mean 37.91 years). Analysis of past treatment revealed that none of these patients had been reassured about the nature of the pain and the absence of serious underlying breast pathology. Twenty-three (43.4%) patients had been prescribed analgesia (non-steroidal anti-inflammatory drugs) and 12 (22.6%) had been prescribed vitamin E. The rest (18 patients) had been treated with danazol, bromocriptine, progesterone, miscellaneous hormone combinations and evening primrose oil (Figure 1). The dose and duration of the treatment was not reliably discernable from the multiple prescriptions issued to most patients by multiple medical practitioners. None of the patients admitted to improvement with past treatment. Clinical breast examination revealed that 34 (64.2%) patients had nodularity in the breasts, 17 (32.1%) had normal breast examination and two patients (3.8%) had a clinical finding of a fibro adenoma (confirmed by FNAC). Investigations in the form of haemogram, thyroid, prolactin and lipid profile assessment revealed no statistically significant abnormalities. At the three-month review, the response to treatment was as follows: In the cyclical mastalgia group, 13 (43.3%) had Grade 1 (excellent) response, 14 (46.7%) had Grade 2 (substantial) response and three (10.0%) had Grade 3 (poor) response. None had Grade 4 (no response). In the non-cyclical mastalgia group, 11 (47.8%) had Grade 1 (excellent) response, ten (43.5%) had Grade 2 (substantial) response and two (8.7%) had Grade 3 (poor) response. None had Grade 4 (no response). At the six-month review, the response to treatment was as follows: In the cyclical mastalgia group, 17 (56.7%) had Grade 1 (excellent) response, 11 (36.7%) had Grade 2 (substantial) response and two (6.7%) had Grade 3 (poor) response. None had Grade 4 (no response). In the non-cyclical mastalgia group, 14 (60.9%) had Grade 1 (excellent) response, eight (34.8%) had Grade 2 (substantial) response and one (4.3%) had Grade 3 (poor) response. None had Grade 4 (no response). At the end of the study, an overall response (Grades 1 or 2) to treatment was seen in 50 (94.3%) patients, (95% CI 86.01 100). Three (5.7%) patients had Grade 3 response (Table 1). It was noted that 46 (86.8%) patients were adhering to monthly breast self-examination and all 53 patients complied with evening primrose oil supplementation. DISCUSSION Because of increasing awareness about breast cancer and the fear that breast pain may be indicative of it, more and more women are seeking treatment for mastalgia. But most clinicians are ill-trained to handle mastalgia. As breast cancer seldom presents with pain,6,7 patients are often dismissed with no formal evaluation, no reassuring explanations and often with a prescription of drugs which have no established therapeutic value or those with irksome or even potentially dangerous side-effects. Such prescription patterns are not unique to India. The management of mastalgia has become increasingly refined and standardized in the hands of specialist surgeons. When confronted with an instance of mastalgia, the treatment protocol adopted takes into account the nature, the source and the duration of pain. In the majority of instances, where the pain is mild to moderate and the duration is short-lived (less than six months), after thorough evaluation, the patient is treated by reassurance only. This consists of an explanation that mastalgia is an aberration and not a disease and that it is not indicative of serious underlying disease. Because of the possibility of spontaneous remission8 (approximately 20% in cyclical mastalgia and 50% in non-cyclical mastalgia), pharmacological management is not indicated. This is effective in 8085% of patients.9 In addition, advice is given on: the use of supportive undergarments, adhering to a low-fat, methyl xanthine restricted diet and abstention from drugs (i.e. oral contraceptive pill or hormone replacement therapy).10 In those instances, where the pain is severe or persistent, in addition to the above steps, evening primrose oil capsules in a therapeutic dose of 3 g /day given orally was until recently the first line drug in the treatment of cyclical mastalgia and true non-cyclical mastalgia. In the U.K. clinical experience, the overall response rate to it was 44% in cyclical pain and 27% in non-cyclical pain.11 Danazol12,13 (overall response 70% in cyclical mastalgia and 31% in non-cyclical pain), bromocriptine14,15 (overall response 47% in cyclical mastalgia and 20% in non-cyclical pain) and tamoxifen16 (overall response 75% differentiation) were reserved for treatment failures. But evening primrose oil does not possess the current standard of therapeutic efficacy (compared to say danazol or tamoxifen) required for marketing authorisation as a drug for the treatment of mastalgia. Indeed it has never been listed in the U.S.A, where danazol is the only drug approved by the FDA for the treatment of mastalgia.17 With effect from October 2002, the U.K. Medicines Control Agency has withdrawn marketing authorisation18 given earlier to evening primrose oil, and new drug protocols for the management of mastalgia are now being drawn up. Evening primrose oil is, however, freely available as a food supplement around the world including India as there are no safety issues regarding its use. In this study, analysis of past treatment revealed that none of the patients had been reassured about the nature of the pain and the absence of serious breast pathology. As reassurance is the cornerstone of the successful treatment of mastalgia, it is not surprising that these women continued to seek further treatment, for what they perceived as a serious problem. Forty patients (75.5%) had received analgesia,19 vitamin E,20 progesterone,21 and miscellaneous hormone combinations22 which are considered non-standard drugs as the literature supporting their use is conflicting and currently inconclusive. Only a minority of the patients had been treated with danazol, bromocriptine and evening primrose oil which are standard drugs used in the treatment of mastalgia. It is to be noted that both danazol and bromocriptine use is fraught with side-effects (22% and 45% respectively) 23 and therefore usage needs to be carefully balanced against the severity of mastalgia. As some of these side-effects may be irreversible or even fatal, their use in first line management, particularly in the primary care set-up cannot be recommended. In the present study patients were treated with a protocol of reassurance, advice on adhering to a low-fat, methyl xanthine restricted diet and dietary supplementation with 500 mg/day of evening primrose oil (not as a therapeutic drug, the dosage of which is 3 g/day). The importance of reassurance in the treatment of mastalgia dictated that it should be the first ingredient in the treatment protocol used. The value of methyl xanthine restriction has not been proven.24 It has been suggested that low-fat diets (15% of total calorie value for prolonged periods) may have a positive impact,25 but the creation of randomized trials have proven difficult in practice owing to lack of patient compliance to a drastic change in dietary habits. Despite lack of concrete evidence, mastalgia patients continue to be given advice on adhering to low-fat, methyl xanthine restricted diets in breast clinics around the world. In this study, while patients were advised to adhere to such a restricted diet as a lifestyle change, no rigid implementation was done nor was it practical to do so in a study of this ambit. The value of dietary supplementation with evening primrose oil remains to be established through randomised control trials. The contribution of the individual components of treatment (reassurance, dietary restriction and supplementation) is impossible to determine in an observational study of this nature. As 50 patients showed Grade 1/2 overall response and only three patients had Grade 3 response at the end of six months, to non-pharmacological treatment, one may say that 50 out of the 53 (94.3%) patients were in fact instances of inadequately treated mastalgia and not refractory mastalgia, thus proving the aim of this study. The study also illustrates without doubt that there is scope for improvement in mastalgia management. ACKNOWLEDGEMENTS The author wishes to acknowledge Dr. B. W. C. Sathiyasekaran, Professor, Department of Community Medicine, Sri Ramachandra Medical College and Research Institute, Porur, Chennai for checking the statistical analysis. REFERENCES
© 2004 Indian Journal of Surgery. The following images related to this document are available:Photo images[is04021t1.jpg] [is04021f1.jpg] |
| |||||||||

{kind=link}
{kind=link}