 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 66, No. 2, Mar-Apr, 2004, pp. 93-96 Classification of thymic neoplasms: Observations on the WHO 1999 classification based on 56 cases Saral S. Desai, Nirmala A. Jambhekar Department of Pathology, Tata Memorial Hospital, Mumbai, India.
Paper Received: November 2003. Paper Accepted: January 2004. Source of Support: Nil. Code Number: is04022 ABSTRACT Background: The World Health Organization (WHO), in
1999, laid down histological criteria for thymoma sub-classification (Type
A, AB, B1, B2, B3 and C). This study aims to assess the ease of application
of this classification and to evaluate any relationship with the clinical stage.
KEY WORDS Thymoma, WHO classification, Myasthenia, Thymus, Tumour. How to cite this article: Desai SS, Jambhekar NA. Classification of thymic neoplasms: Observations on the WHO 1999 classification based on 56 cases. Indian J Surg 2004;66:93-6. INTRODUCTION The diagnosis and classification of primary thymic epithelial neoplasms has been a source of major difficulty for surgical pathologists owing to the rarity and broad range of the morphological appearances of these tumours. Thymomas have mirrored lymphomas in their morphological complexity and the numerous classification schemes proposed over the years based either on morphological,1-8 or clinical,1,9,10 or histogenetic considerations,3,11 bear testimony to this fact. Ideally, a good classification should be reproducible and clinically relevant. The WHO proposed a new classification for Thymic Neoplasms in 1999.12 The present study was undertaken to re-classify thymic neoplasms as per the WHO Classification, with a view to assess the ease of application and to evaluate whether any relationship exists with the clinical stage. MATERIAL AND METHODS A search of the surgical pathology records at our hospital, for the period 1994 to 2000 was conducted to retrieve cases of thymic neoplasms. A total of 60 thymic neoplasms were recorded. The surgical pathology material received was in the form of primary tumour excision (31 cases) or submission of paraffin blocks of cases operated in other hospitals (rest of the cases). There was no autopsy material. Demographic data, stage and treatment modalities were noted from the patients' files. Routine histological sections were prepared from 10% formalin-fixed, paraffin-embedded tissue sections, stained with haematoxylin and eosin. The tumours were classified as per the WHO Classification wherein the morphology of the epithelial cells, presence of an organo-typical pattern and proportion of lymphocytes form the basis of the classification. To state briefly, Type A tumours have spindle or oval-shaped cells and Type B tumours have round or polygonal cells. Type AB has a mixture of Type A and B. The B1 tumours have areas resembling the cortex and medulla of a normal functional thymus, B2 has scattered epithelial cells with no atypia and dense lymphocytic infiltrate and B3 has epithelial cells with nuclear atypia and relatively sparse lymphocytes. And finally, Type C tumours are frank carcinomas (which are recognizable as either squamous carcinoma, mucoepidermoid carcinoma, etc.). For the sake of clarity and continuity with the previously widely used histogenetic classification,11 the equivalents in the WHO classification are as follows: Type A medullary thymoma, Type AB mixed thymoma, Type B1 predominantly cortical thymoma, Type B2 cortical thymoma, Type B3 well-differentiated thymic carcinoma, and Type C thymic carcinoma. The tumours were staged according to the Masaoka Staging System,13 which briefly put, is as follows: Stage I Macroscopically, completely encapsulated and microscopically, no capsular invasion Stage II
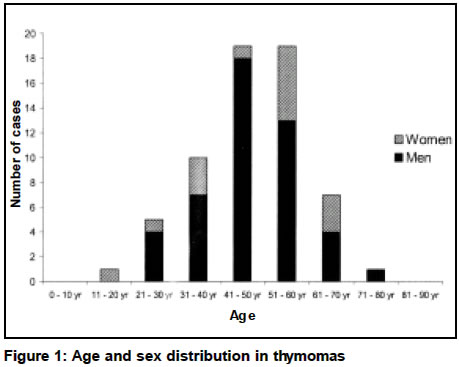
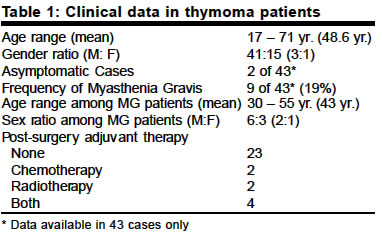
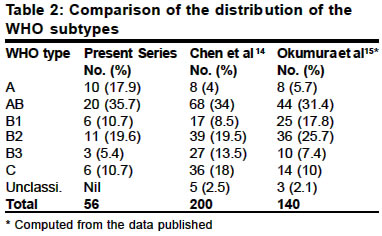
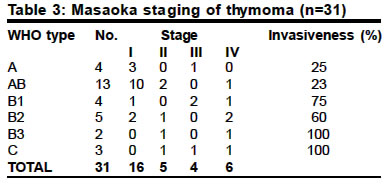
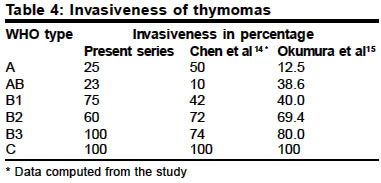
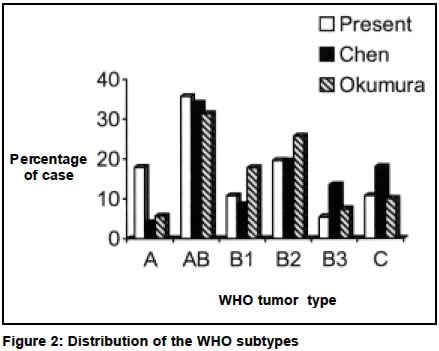
Stage III Macroscopic invasion into neighbouring organs (pericardium, great vessels and lung) Stage IVa Pleural or pericardial dissemination Stage IVb Lymphogenous or haematogenous metastasis RESULTS In the 7-year period, a total of 60 cases of thymic neoplasms were studied. Of these, 56 cases were classified as thymomas and thymic carcinomas and 4 cases were classified as neuroendocrine tumours. The age and gender distribution is depicted in Figure 1 and 80% of the patients were in the 40 to 60 age group. The clinical data is summarized in Table 1. Myasthenia Gravis was noted in 9 of the 43 cases in which the history was available. Pathology The tumour size ranged from 3 cm to 34 cm with an average of 9.8 cm. These tumours were encapsulated and a breach in capsule was seen in 6 cases. A majority of the tumours were solid, 9 were both solid and cystic, and 3 were purely cystic. The cut surface had a white to tan colour and a lobulated appearance. Histologically, the distribution of the WHO subtypes was as follows: Type A 10 cases, Type AB 20 cases, Type B1 6 cases, Type B2 11 cases, Type B3 3 cases, and Type C 6 cases (Table 2). The incidence of Myasthenia Gravis which was noted in 9 of 43 tumours was as follows: Type A 1 case, Type AB 4 cases, Type B1 1 case, Type B2 2 cases, Type B3 none, and Type C 1 case. Adequate information for the Masaoka staging was available in only 31 cases that were operated at the institute (Table 3). In the remaining cases the clinical, operative and pathological information was inadequate to stage the tumours. It was noted that there was a definite relationship between the WHO type and the percentage of invasiveness (p < 0.02). DISCUSSION Thymomas are not common tumours. They comprise varying proportions of lymphocytes and epithelial cells. The epithelial cells vary from spindle to polygonal and cytologically they may be benign, atypical or overtly malignant. A combination of these features, and the various patterns associated with thymomas, viz. storiform, cystic, hemangiopericytomatous, trabecular, etc. result in a wide gamut of morphological appearances. This has spurred numerous publications proposing various classification schemes. For a pathologist, a morphological classification scheme which is easy to apply and reproducible would be appealing whereas to a clinician, a classification with clinical relevance and prognostic implications would be of more value. In this study, the clinical features, histology, and tumour stage have been analysed with reference to the WHO Classification. The first part of this discussion deals with our observations regarding the ease of application of this classification. In the second part, the present data is compared with two recent articles14,15 wherein this classification has been used. From a morphologist's point of view, it was observed that it was easy to assign Type AB and Type C subtypes, since the former is essentially a mixture of cells, whereas the latter comprises distinct type of carcinomas (squamous, sarcomatoid, adenocarcinoma, mucoepidermoid, etc.). Regarding the other subtypes, (i) distinguishing oval cells (by definition Type A cells) and round / polygonal cells (by definition Type B cells) was not always easy. (ii) Also the distinction between Type B1 and B2 is on the basis of an organoid pattern (B1), which may not always be easily evident. Since there is no provision for tumours with no epithelial atypia and sparse lymphocytic infiltrate, such tumours were classified as B2. Assigning the correct WHO type was particularly difficult while separating B2 and B3 because the character and the quantification of nuclear / cytologic atypia in B3 has not been elaborated in sufficient detail. Whereas Type B3 has been stated to have only mild atypia in the WHO 1999 Classification, an earlier publication16 states "only tumours exhibiting a clear-cut predominance (more than 50%) of epithelial rich areas with epidermoid differentiation were classified as well-differentiated thymic carcinoma". A more current paper14 investigating the applicability and clinical significance of the WHO Classification has used a 30% cut-off level, wherein B2 tumours with 30% or more of B3 component were typed B3 and combined tumours (B3 and C) with Type C component less than 30% were also typed B3. This is in contrast to the classification and grading schemes for tumours in general, wherein high-grade foci determine the subtype regardless of its quantity. It would be easier to apply the WHO Classification if the same rule were followed (e.g., tumour of Type B3 with small amount of unequivocal squamous carcinoma should be assigned as Type C). Despite these "difficulties", the cases in various histological subtypes were comparable with the data published in the literature (Table 2). Whether the uniformly higher frequency of incidence of subtype AB in all the three studies is a reflection of its true number or merely represents over-interpretation due to reasons cited above is a moot question. The present study does not reveal any relationship between the age and gender of the patient and the WHO tumour subtype. In spite of certain aforementioned problems, the classification was not difficult to apply in practice. Regarding the clinical relevance of the WHO classification, it was found that a definite relationship between the WHO subtype and percentage of invasiveness was observed in all the three studies (Table 4 and Figure 2). It can thus be inferred that the WHO histological subtype correlates well with the risk of invasiveness. Thus despite some minor problems noted in objectively assigning the WHO subtypes, the following conclusions can be drawn from this study: (i) the classification criteria were not difficult to apply, and the frequency of tumour subtypes was similar to that in the published data.14,15 (ii) There is a good correlation between the WHO subtypes and the occurrence of invasive tumour. Hence the WHO 1999 Classification is histologically applicable and clinically relevant. REFERENCES
© 2004 Indian Journal of Surgery. The following images related to this document are available:Photo images[is04022t3.jpg] [is04022f1.jpg] [is04022t1.jpg] [is04022t2.jpg] [is04022f2.jpg] [is04022t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}