 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 66, No. 2, Mar-Apr, 2004, pp. 106-108 Case Report Ileal duplication presenting with peptic ulcer perforation and malena Robbie K. George, Navneet Kaur, V. R. Minocha Department of Surgery, University College of Medical Sciences and Guru Tegh
Bahadur Hospital, Delhi - 110095, India.
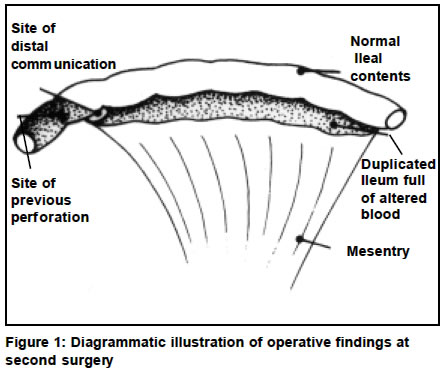
Paper Received: November 2002. Paper Accepted: February 2003. Source of Support: Nil. Code Number: is04026 ABSTRACT Duplications of the alimentary tract are rare congenital malformations and may be found anywhere along the alimentary tract. Their importance lies in the fact that they readily mimic other surgical disease processes and may result in significant morbidity if left untreated. We report a case of ileal duplication with heterotopic gastric mucosa presenting with melena and peptic ulcer perforation and discuss the problems encountered in its management. KEY WORDS Gut duplication, Peptic ulcer perforation peritonitis, Malena. How to cite this article: George RK, Kaur N, Minocha VR. Ileal duplication presenting with peptic ulcer perforation and malena. Indian J Surg 2004;66:106-8. INTRODUCTION Duplications of the alimentary tract are rare congenital malformations and may be found anywhere along the alimentary tract. Their importance lies in the fact that they readily mimic other surgical disease processes and may result in significant morbidity if left untreated. We report a case of ileal duplication with heterotopic gastric mucosa presenting with melena and peptic ulcer perforation and discuss the problems encountered in its management. CASE REPORT An 8-month-old male child presented with complaints of high grade fever and passage of black coloured tarry stools for 6 days. On examination he was markedly pale with abdominal distension, guarding and rigidity. X ray abdomen in erect position showed pneumoperitoneum. Hemoglobin was 2.1 gm/dl and serum widal titres were negative. A provisional diagnosis of typhoid ulcer perforation peritonitis was made. He received 200ml packed cell transfusion and underwent an exploratory laparotomy the same night. At laparotomy an ileal perforation of 0.2 cm diameter was found on the anti mesenteric border of the mid ileum. Three feet of bowel proximal to this point was duplicated as a tubular segment lying on its mesenteric aspect. It was communicating with the distal normal bowel. A biopsy was taken from the edge of ulcer and primary closure of the perforation was done. Definitive resection was considered but was abandoned due to the poor general condition of the child. The patient continued to have melena with features of coagulopathy. The coagulopathy was considered consistent with septicemia, and was treated with transfusions of packed cells and plasma. The melena stopped after 6 days and the child made an uneventful recovery. An elective resection was planned but the child was lost to follow up. He presented again after 4 months with melena and anemia. Nasogastric aspirates were clear. A Technetium99m labeled scan was done and showed a lesion suggestive of heterotopic gastric mucosa at mid ileum. The child was started on ranitidine and hematinics but significant bleeding continued. He underwent a laparotomy again. The duplicated ileal loop and the normal ileum distal to it were found to be full of altered blood (Figure 1). The duplicated segment and adjacent bowel were resected. Bowel continuity was restored by performing a single layer anastomoses. Macroscopic examination showed altered blood originating at the proximal end of the duplicated segment and draining into the normal gut through a 2cm diameter communication at the distal end. Histological examination revealed heterotopic gastric mucosa lining the proximal portion of the duplicated segment. The infant made an uneventful recovery. DISCUSSION The small bowel is the commonest site of alimentary tract duplication and most patients present within the first year of life.1,2 Duplications are slightly commoner in males.1 Duplications may be saccular or tubular, the latter being known to communicate with normal bowel. Histologically duplications have a well-developed smooth muscle wall and inner mucosal membrane. Any type of gastrointestinal mucosa including gastric mucosa may be found. Heterotopic gastric mucosa is found in 29%-60% of cases.1,3,4 Children may present with abdominal mass, distension, pain, vomiting, melena, perforation or obstruction.1,2,5 Diagnosis is commonly made at laparotomy in those presenting acutely, as in our patient. Melena occurs in 20%-35% of patients3,4 but perforation is uncommon.1,5 The bowel perforation may occur in the duplication itself, or very rarely in the adjacent normal intestine that is exposed to acid secreted by the ectopic gastric mucosa. In saccular duplications perforation may be due to the pressure of accumulating intestinal secretions. In those presenting with melena the diagnosis is rarely suspected unless a duplicated segment is found on an ultrasound or barium study. When suspected, a Technetium 99m study helps identify ectopic gastric mucosa within the duplication. However it may not be possible to distinguish from ectopic mucosa in a Meckels diverticulum, another cause of melena. Short duplications are best treated by resection and primary end to end anastomoses. If complete excision is impossible, long duplications may be separately excised while preserving normal gut. Alternatively the duplication can be partially excised with the remnant stripped of mucosa, but this may be difficult in some cases, as vascularity of the remaining bowel may be compromised.1 This child presented initially with ileal perforation and melena. The perforation was probably secondary to exposure of normal intestinal epithelium to acid secreted by the heterotopic gastric mucosa within the duplicated bowel. As resection was not possible at the time of first operation an elective resection was planned. It could not be carried out as the child was lost to follow up. In retrospect, it might have been better to carry out elective resection of duplicated gut during the first admission itself. This case highlights the emergency presentation of gut duplication and the problems associated with its management. REFERENCES
© 2004 Indian Journal of Surgery. The following images related to this document are available:Photo images[is04026f1.jpg] |
| |||||||||

{kind=link}