 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 66, No. 2, Mar-Apr, 2004, pp. 119-120 Images in Surgery Barium meal-induced gastric perforation Siddharth Lakhotia, G. P. Shrivastava Department of Surgery, S. S. Medical College & Associated G. M. and S.
G. M. Hospitals, Rewa, India.
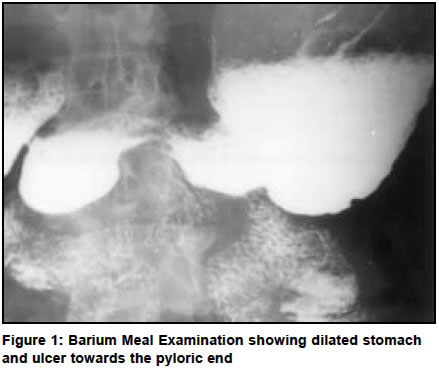
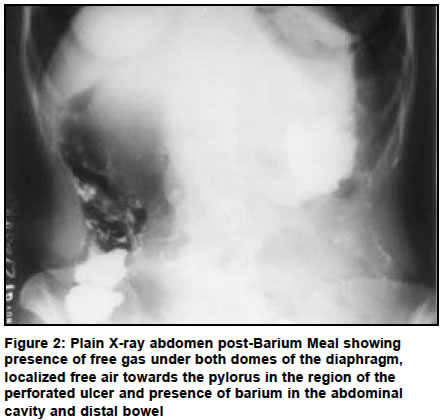
Paper Received: June 2003. Paper Accepted: October 2003. Source of Support: Nil. Code Number: is04032 How to cite this article: Lakhotia S, Shrivastava GP. Barium meal-induced gastric perforation. Indian J Surg 2004;66:119-20. A 56-year-old woman was admitted with 24 hour history of pain all over the abdomen and not having passed stool and flatus. She had history of pain in the upper abdomen for last 6 months, anorexia and vomiting after meals for last 4 months. A day before, in the morning, she was subjected to Barium Meal Examination which showed dilated stomach with filling defect towards the pylorus, indicative of ulcer and gastric outlet obstruction (Figure 1). Exacerbation of abdominal pain occurred six hours after Barium Meal Examination. Abdominal examination revealed generalized guarding and tenderness. Distension and bowel sounds were absent. A plain X-ray abdomen done in upright position approximately 30 h after Barium Meal showed presence of free gas under both domes of the diaphragm, localized free air towards the pylorus in the region of the perforated ulcer and presence of barium in the abdominal cavity and distal bowel (Figure 2). At surgery, the patient was found to have a perforation in the pyloric region of the stomach and contamination of the peritoneal cavity by barium (Figure 3) along with about 500 ml of reactive peritoneal fluid. Closure of perforation was done with omentopexy. After thorough peritoneal lavage, the abdominal cavity was closed with a drain in the peritoneal cavity. The postoperative period was uneventful and she was discharged on the 10th postoperative day. Barium Meal of stomach and duodenum are commonly performed for the evaluation of the stomach and duodenum. Rarely, such procedures may lead to life-threatening complications. Rosenthal was the first person to report a case of barium peritonitis in 1916.1 Barium sulphate being a suspension instead of solution is not absorbed but is only phagocytosed slowly. Barium perforation in acute stage may lead to peritoneal fluid accumulation and shock2 and in chronic phase may cause adhesions, recurrent episodes of bowel obstructions and barium granuloma formation. Mortality rates for barium peritonitis either after barium meal or after barium enema are very high. Early administration of large amounts of IV fluids along with parenteral antibiotics, urgent laparotomy and perforation closure with thorough irrigation of the peritoneal cavity with Normal Saline combined with removal of the greater omentum removes the largest quantity of barium. However, if the patient is unfit for laparotomy then intraperitoneal drain should be put under local anaesthesia. In barium peritonitis secondary to barium enema, antibiotics and vigorous fluid therapy, alone or with simple cecostomy should be adopted in patients who are considered poor surgical risks.3 REFRENCES
© 2004 Indian Journal of Surgery. The following images related to this document are available:Photo images[is04032f2.jpg] [is04032f1.jpg] [is04032f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}