 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
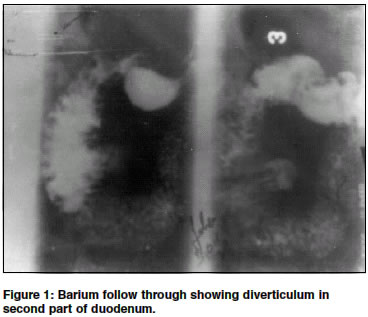
Indian Journal of Surgery, Vol. 66, No. 3, June, 2004, pp. 140-145 Review Article Duodenal diverticulum: Review of literature Mahajan Sanjay K, Kashyap Rajesh , Chandel Upender K, Mokta Jatinder , Minhas Satinder S Department of Medicine, Indira Gandhi Medical College, Shimla - 171001 Code Number: is04035 ABSTRACT Duodenal Diverticulum was first reported by Chomell in 1710 and was regarded an anatomic curiosity until 1913 when first radiological demonstration was done by JT Case. With modern radiological techniques and widespread use of endoscope it has been found that these diverticula occur more frequently than was formely supposed. Most of these are asymptomatic, situated in second part of duodenam and are rarely associated with complication which are usually cause of presentation.INTRODUCTION Duodenal diverticula was first reported by Chomall in 1710 and first well documented report was made by Morgagni in 1762 and it was regarded an anatomic curiosity until 1913 when radiological demonstration was done by JT Case, who displayed roentgenograms of 4 cases in the Scientific Exhibit of the American Medical Association. With lengthening of life span, diverticulosis has come to occupy a more important position in the sphere of clinical gastroenterology. Duodenum is second most common site of diverticula in alimentary tract after colon followed by jejunum, ileum and stomach.[2],[3] Duodenal diverticula are found in up to 25% of patients, but rarely cause symptoms when complications occur, early diagnosis is essential if treatment is to be successful.[3] Diverticula of duodenum are classified as primary and secondary. Majority of secondary or false diverticula are result of chronic duodenal ulceration, so called prestenotic diverticulum where as primary are true diverticula.[4] These occur mainly in later decades of life with peak incidence between 50 and 60 years of age and it increases with age.[1],[2],[4],[5],[6] There is no gender predisposition but female preponderance has also been reported.[1]-[5] Incidences varies with diagnostic method used.[3] In UGI barium series it is 0.016 to 6%,[2],[4],[5],[6],[7],[8] in autopsy series 22 to 23%,[2],[4],[5],[7] where as on ERCP studies incidence is 9 to 23%.[6],[7] Over 95% of duodenal diverticula project from inner or pancreatic border of duodenal curve in second, third and fourth parts. Second part is most common site with 85 to 90% of total DD.[1],[2],[4],[9] Third and fourth parts of duodenum have 20 and 10% of diverticula respectively,[2] but up to 30 to 40% of these may arise from third and fourth part of duodenum.[10] Diverticulum may be single or multiple and as many as 6 or more has been reported. Incidence of multiplicity at x-ray series is 1.4 to 23.5% and in autopsy series it is 3.5 to 30%. These are usually spherical or hemispherical and when filled with barium usually oval in shape often resembling Erlenmeyer flask showing narrow neck.[2] These are classified into EDD and IDD. EDD are more common[3] and can be further classified into PAD and JPDD. PADS are extra luminal mucosal out pouching of duodenum arising adjacent to or containing the ampulla of Vater or intraluminal portion of CBD (common bile duct). JPDD are defined as EDD located with in radius of 2 cm of major papilla but not containing it. Some has referred to above definition as ampullary and periampullary while others refer both type of EDD collectively as JPDD. However, consistent and precise terminology needs to establish. About 75% of EDD occur with in 2 cm of ampulla of Vater.[2]-[6],[10],[11],[12] AETIOLOGY AND PATHOLOGY These are true pouches or sacs protruding from duodenal lumen not caused by any recognizable intrinsic or extrinsic disease. EDD are acquired and consist of a sac of mucosal or sub mucosal layers herniated through a muscular defect in bowel wall but precise manner of the development is not known.[2],[6],[10] However, there exists a locus minoris resistentiae which may be created by (i) passage of the biliary, pancreatic duct and blood vessels through the wall of duodenum. (ii) Congenital absence of an adequate muscle coat (iii) heterotrophic pancreatic tissue. Once diverticulum is formed it may increase in size through the years.[2],[6],[10] The position of fundus and body of EDD is variable and mostly lie in retro peritoneum with large portion lying close to concave medial surface close to CBD and pancreatic duct. Rarely, the diverticula may be localized on the convex side of the second part of duodenum. The sac lie along side, extend behind or even penetrate into the pancreas and occasionally CBD and duct of Wirsung may open into the diverticulum[3],[4],[6] IDD or windsock diverticula are not true diverticula and occur as single saccular structure which are connected to the entire circumference or only part of the wall of the duodenum. Only less than 100 cases have been reported in the literature. During early foetal life duodenal lumen is initially occluded by proliferating epithelial cells and recanalises later on. Abnormal recanalising may lead to a duodenal diaphragm or web which may not produce symptoms in child hood however over the period of time peristaltic stretching may transform it into an IDD. IDD may project as distally as fourth part of duodenum and often a second opening is located eccentrically in the sac and both sides of the diverticulum are lined by mucosa.[3],[6],[10]Pathologically the larger pouches usually lack a muscular coat although often the smaller one do contain some fibers. Attempts have been made to divide duodenum diverticulum in to true or congenital pouches and false or acquired pouches. If all muscle coats are presents it was termed true or congenital and if muscle layer was not present it was thought to be acquired or false, such a division seems untenable as there is nothing to prove that certain pouches are basically congenital and others entirely acquired. The amount of muscle fibers in the pouch depends more upon its age and size. Histologically in majority, the circular and longitudinal muscle coats of duodenum are missing and the mucosa and muscularis mucosae make up the wall of the diverticulum.[2] CLINICAL FEATURES Great majority of duodenal diverticula are asymptomatic.[2],[4],[6],[7],[9],[10] Clinical presentation may be characterized by non-specific abdominal symptoms[4] and less than 5% of patients have abdominal symptoms.[2] Abdominal discomfort is usually located in epigastrium, right upper abdomen or umbilical area which is made worse or brought on by eating and relieved by vomiting, belching or assuming certain posture.[2],[4],[6] There are no characteristic symptom complex from which one may make a positive diagnosis of DD. Many believe that there are three main factors in production of symptoms.A. Mechanical causes producing Patients may complain of pain radiating to the back between the scapulae and between costo-vertebral angles. The pain caused by the diverticula in the third part of the duodenum is situated near the mid line where as that caused by the pressure upon the pancreas may be situated to the left. The peptic ulcer like syndrome has been noted in several patients, however in the absence of ulcers, the symptoms may be due to inflammation and stasis in the sac. The simulation of peptic ulcer disease by DD may be close. Intermittent diarrhea and constipation, weight loss because of the fear of eating and steatorrhea may also occur in some patients.[2],[3],[10],[11] The symptoms simulating primary biliary tract disease may occur in DD located near ampulla of Vater and some time CBD may terminate in the diverticulum. The "perivaterian diverticulitis" may give rise to obstructive jaundice. The greater propensity for the pigment stones in the presence of EDD is not fully understood and excess release of calcium bilirubinate by ascending Beta-Lucuronidase colonization into CBD has been the possible cause.[2],[3],[5] Several authors have shown that compression of CBD, dysfunctions of ampulla or a poorly emptying diverticulum with a narrow neck can lead to pancreatico-biliary disease and acute pancreatitis. Some even suggested that PAD be included in the aetiology of acute pancreatitis especially in the elderly.[13] JPDD are important causative factors in the bile duct stone formation.[14],[15] Since choledocholithasis leading to biliary obstruction is a well known etiology of acute pancreatitis there is debate whether the increased incidence of pancreatitis with EDD is due primarily to the mechanical complications or associated biliary stones. As most DD occur on the concave border of second part of duodenum in close contact with or embedded in to the head of pancreas, perforation of diverticulum can also cause pancreatitis.[2],[5],[6] The majority of IDD, in contrast to EDD, will become symptomatic and can present at any age from the first through the eighth decade of life. The most common symptoms are those of incomplete duodenal obstruction by retention of vegetable or foreign bodies. Pancreatitis and hemorrhage has also been reported in IDD. In childhood cases 20% can have symptoms and it is to be differentiated from duodenal intrinsic defect, extrinsic defects, and anal rotation with congenital bands.[3],[6],[10],[16] Complications As diverticula are usually asymptomatic, complications are responsible for presentation most of the times.[11] The complications may be divided into two groups. Those related to pressure on the adjacent structures and those caused by inflammation. Jaundice, cholangitis, acute and chronic pancreatitis and duodenal obstruction are caused as a result of mechanical compression by diverticula, whereas diverticulitis and ulceration are caused by inflammation.[2],[3],[4],[6],[10],[11]Diverticulitis and Perforation Ulceration can occur because of presence of ectopic gastric mucosa or inflammation. Diverticular ulceration may give rise to massive bleeding or perforation into aorta or a mesenteric vessel. The intake of NSAIDs has also been attributed to ulcerations or hemorrhage.[2],[3],[10],[11],[17] Although it is extremely uncommon nevertheless massive GI hemorrhage leading to shock can be due to diverticula.[2],[9],[11],[12] Some believe that bleeding from diverticula is more common than thought, and index of suspicion should be raised in UGI hemorrhage where causes have been excluded by endoscopy.[2],[7] Duodeno-colic, gastro-jejuno colic fistula formation may occur secondary to inflammation in diverticula. Pancreatic and / or biliary fistula as a complication during surgery has also been reported. Intestinal obstruction as a result of blockage of the distal part of the bowel by a large calculus (enteroliths) which has been extruded from a DD has been reported. Neoplastic changes including adenocarcinoma, sarcoma, leiomyosarcoma or fibroma is also known. Peridiverticulitis and bezoar formation are other complication described with this condition.[2],[3],[6],[10] Associated diseases Duodenal ulcerIt has been noted in large number of patients with DD. A suspicion of duodenal ulcer has been principal reason for subjecting many patients to investigation. Although relationship of duodenal ulcer with DD is important one, there does not seem to be any cause and effect relationship.[2],[3],[10] Hiatus Hernia Diverticula elsewhere DIAGNOSIS Upper GI barium studiesDuodenal diverticulum is an incidental finding of UGI barium examination after ingestion of barium, study is made in erect, recumbent and oblique positions. One of most important feature is abnormal retention of barium in the sac. Barium retention for 6 or more hours is diagnostic. The use of a small amount of barium may help to avoid the overlapping of duodenum by jejunal loops and by the completely filled stomach. At times sac is better visualized from 1-2 hours following the opaque meals.[2],[4],[6],[10],[18] Differential diagnosis barium upper GI series In upper GI series in patients with IDD, the "duodenal Wind Sock sign" may be seen. It consists of barium filled sac that lies entirely within duodenum and is surrounded by a narrow radio-luscent line which is well demonstrated as the barium in the duodenum passes distal to the diverticulum.[16] Upper G.I. Endoscopy is an important investigation for diagnosis of DD. It is successful in diagnosing DD in more than 75% of patients.[19] Side viewing endoscopy may further increase the success rate. The rate of failure of endoscopy to diagnose DD may increase if DD is situated in third or fourth part of the duodenum. At endoscopy IDD appears as a sac like structure with eccentric aperture lying with normal mucosa or as a soft polypoidal mass.[6],[16] JPDD make endoscopic examination as well as possible subsequent intervention more difficult. Guide wires should be used for complicated procedures. Diverticula may even be the cause of failure or complications such as hemorrhage or perforations. It can also diagnose associated lesions which may be responsible for symptoms. But it has also failed to identify bleeding diverticula in up to 70%[7] few other studies have also highlighted the failure of endoscopy to diagnose bleeding diverticulum and more so when it was situated in third or fourth part of duodenum.[7],[9],[10],[11] ERCP (Endoscopic Retrograde Cholangiopancreatography) when done for investigating pancreatico-biliary system can diagnose large number of diverticula.[6],[7],[12],[20] Whenever endoscopy can not determine the cause of bleeding, angiography may be performed.[7],[21] Diagnosis can also be established with combination of arteriography and scanning with Technetium-99 lebelled red cells.[7],[9] CT scan and MRI
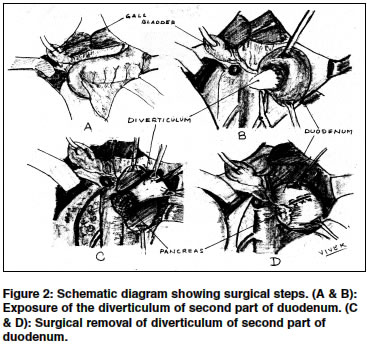
Treatment Surgical excision is not without complications and mortality rate of 30% in post operative period has been reported. A delay in diagnosis can lead to perforation in DD which carries a mortality rate of 90%.[10] Injury to adjacent ampulla of Vater leading to interference with drainage of bile or pancreatic secretions may lead to jaundice, pancreatitis, or development of duodenal fistula. An overaggressive attempt to dissect the duodenum from pancreas may lead to pancreatitis and hemorrhage. Laparoscopic duodenal diverticulectomy can be done by using intraoperative endoscopic guidance.[27],[28],[29],[30] All IDD require treatment as recurrence of symptoms is certain. Curative treatment consists of removal of diverticulum by laparotomy and duodenotomy or by endoscopy. If diverticulum is not circumferentially attached, it can be resected endoscopically with an electrocautery snare. If it is attached circumferentially it can be inverted with the endoscope, partially resected to create an opening in the blind end. When papilla, CBD, or pancreatic duct cannot be clearly identified duodenostomy should be performed. If at the time of duodenotomy the papilla cannot be identified, choledochotomy and placement of a bile duct probe to localize the papilla should be performed prior to the resection of the diverticulum.[3],[4],[10] Duodenal diverticulum present in about 25% of patients. DD can be commoner than EDD, which are acquired or IDD which are congenital and rare. Majority are asymptomatic, only a small percentage of patients will develop symptoms ranging from mild abdominal discomfort to serious complications like diverticulitis, perforation, ulceration and haemorrhage. Majority of diverticula can be diagnosed by endoscopy, especially side viewing endoscopy and upper GI barium studies. Asymptomatic diverticula do not require surgical management. Surgical procedures in this area are difficult to perform and are associated with high rate of post-operative complications and mortality. Early recognition is essential if treatment is to be successful. REFERENCES
Copyright 2004 - Indian Journal of Surgery The following images related to this document are available:Photo images[is04035f2.jpg] [is04035f1.jpg] |
| |||||||||

{kind=link}
{kind=link}