
|
Indian Journal of Surgery
Medknow Publications on behalf of Association of Surgeons of India
ISSN: 0972-2068
Vol. 66, Num. 3, 2004, pp. 146-151
|
Indian Journal of Surgery, Vol. 66, No. 3, June, 2004, pp. 146-151
Review Article
Latrogenic splenic injury: Prevention and treatment
Sharma Dhananjaya
Incharge GI Surgery Unit, Govt. NSCB Medical College and Allied Hospitals, Jabalpur-482003
Correspondence Address:31/3, US Club, Shimla-171001
sanjay_mahajan64@rediffmail.com
Code Number: is04036
Accidental or iatrogenic splenic injury during other abdominal operations is neither infrequent nor inconsequential. Awareness of the hematological and immunological consequences of splenectomy has led to a significant change in surgical philosophy and has resulted in with emphasis on splenic preservation. It is well known that accidental splenectomy leads to significantly higher transfusion requirements, significantly longer mean length of hospital stay and significantly higher prevalence of infectious complications, regardless of the type of operative procedure.[1],[2],[3],[4],[5],[6],[7],[8] Even more important is the fact that accidental splenectomy is associated with the highest mortality among different indications of splenectomy (Accidental Splenectomy > external trauma > hematological).[9],[10],[11] All this makes it mandatory on the part of operating surgeon to ensure that there is no iatrogenic splenic injury. This article is a brief review of etiology, technical tips on how to prevent and treat iatrogenic splenic injury. Incidence
Iatrogenic injury to the spleen is a well known complication of abdominal surgery but the extent of the problem is often under-estimated; which may be due to failure to report splenic injury on the operation note or inaccurate recording of the indication for splenectomy. Splenectomy for iatrogenic injury may be recorded as being part of a radical cancer procedure or to facilitate exposure in procedures for benign lesions.[12] Not surprisingly, surgeons have been known to avoid admitting a splenectomy for iatrogenic trauma.[13] Iatrogenic splenic trauma has been reported as the cause of 9-40% of all splenectomies.[4],[14],[15],[16] Its reported incidence during different surgical procedures is as follows: gastro-esophageal operations (vagotomy, gastrectomy, trans-hiatal oesophagectomy, anti-reflux procedures) 2-9%, splenic flexure mobilization 1.2-8%, vascular operations (abdominal aortic aneurysm repairs, thoracoabdominal aneurysm repair, left renal artery bypass, and reconstruction of the proximal abdominal aorta and its major branches) 0.5-5%, left nephrectomy 1.4-24%, and bariatric surgery 3%.[2],[3],[5],[7],[8],[16],[17],[18],[19],[20],[21],[22],[23],[24],[25],[26] Rarely, spleen gets damaged during drainage of subphrenic abscess, gynecological operations due to traction during omentectomy, left sided thoracocentesis, percutaneous renal biopsy, percutaneous nephrolithotomy and adrenalectomy. An excellent review of various operative procedures leading to iatrogenic splenic trauma has been recently published.[12] Etiology and mechanism of injury to spleen
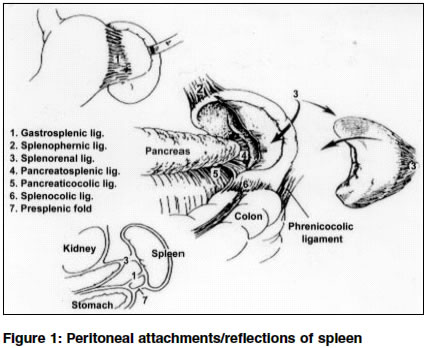
The spleen is rather firmly attached in the left upper quadrant by eight ligaments or peritoneal reflections:[27]
1. Gastro-splenic (containing short gastric blood vessels)
2. Spleno-renal (containing splenic blood vessels)
3. Spleno-phrenic
4. Spleno-colic
5. Pre-splenic folds
6. Pancreatico-splenic
7. Phrenico-colic
8. Pancreatico- colic [Figure - 1]
The spleen may be injured in three ways: Traction, application of retractors or directly by the surgeon′s instruments.[12] Traction is the commonest mechanism of injury. Excessive manipulation or unnecessary traction on perisplenic peritoneal folds result in tear of splenic capsule and / or pedicle; a fact known courtesy anatomical study of numerous peritoneal attachments of the spleen.[28],[29] As can be expected, spleen is at a high risk for accidental injury during operations performed in the left hypochondrium and improper/ inadvertent traction during mobilization of stomach, omentum and splenic flexure are commonest surgical mistakes leading to avulsion of peritoneal attachments. The use of retractors can also cause injury to the spleen, either directly or indirectly through excessive traction on the abdominal wall.[18] Direct injury to the spleen by the operating surgeon, although possible, is rarely reported. Types of injuries
Capsular tears, lacerations, avulsions and subcapsular haematomas are the injuries most frequently encountered; capsular tears being the commonest and the lower pole of the spleen appears to bear the brunt in most cases.[12] This is not surprising as most injuries are caused by traction on peritoneal attachments to the spleen, which are concentrated at the lower pole.[15] Risk factors for iatrogenic splenic trauma
Previous surgery
Understandably, risk of splenic injury is significantly higher if the patient has had previous abdominal surgery, particularly in the left upper quadrant.[16],[29],[30],[31] This increased risk is due to the development of dense adhesions in the left upper quadrant of the abdomen. Traction on various structures indirectly causes traction on the splenic capsule, through these adhesions, resulting in splenic injury. Difficult dissection of these adhesions to obtain exposure and to free structures may also result in direct injury to the spleen.[12]Type of surgical incision
As expected, poor exposure with a ′inadequate′ incision is a contributing factor to splenic injury.[3],[13] In the case of a left nephrectomy, the risk of splenic injury is much higher with a transperitoneal compared with an extraperitoneal approach.[19] Nature of pathology
Splenic injury is more likely if the indication for surgery is malignant disease of left kidney, with a large growth on the upper pole.[19],[20] Similarly, mobilization of a densely adhered splenic flexure may give rise to accidental splenic trauma.[17] Pathology in the spleen
Most of the spleens removed incidentally are grossly and microscopically unremarkable; and the lacerations result from excessive manipulation rather than any pathological changes predisposing to rupture but splenic pathology can increase the risk of iatrogenic trauma. A large spleen will be a predisposing factor as it will come in way of other procedures and is more likely to be damaged inadvertently. Similarly, splenomegaly as a result of portal hypertension is more likely to get injured; not only due to its size and vascularity but also due to traction/retraction trauma to its various extra-anatomical (e.g. to diaphragm, to retroperitoneum) vascular adhesions. Tendency of congestive/infective splenomegaly to rupture with even insignificant trauma is well known. Patient characteristics
Obesity, with its attendant inadequate exposure and non-resilient parietal reflections, leads to increased risk of inadvertent splenic trauma.[32] Increased friability of the spleen secondary to degenerative vascular disease, as well as lack of rib elasticity, leading to over vigorous retraction of the left costal margin, gives rise to increased incidence of iatrogenic splenic injury in elderly patients.[29],[30],[33] Prevention
Constant awareness of the problem and continued vigilance based on knowledge of anatomic relationships is the key to prevention of iatrogenic splenic trauma. Additionally, good exposure and adequate visualization are the two cornerstones of neat and clean surgery. Nowhere are these basics more important than in avoiding inadvertent trauma to spleen. Good exposure by appropriate incision
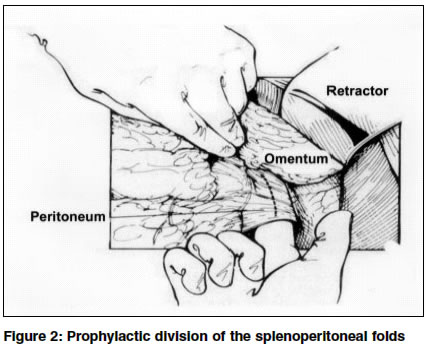
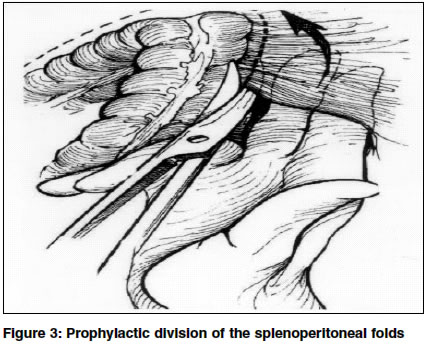
First and foremost prerequisite for good exposure is the planning of appropriate surgical incision (remember the old aphorism you can do it properly if you can see it properly). An inadequate incision is more likely to result in traction to various splenic folds leading to capsular or hilar tears.[3] Superiority, vis-a-vis, exposure by large left subcostal and bilateral subcostal approach with a T-vertical cephalad extension (Mercedes Benz incision)has been shown over midline incision for left nephrectomy.[20],[34] In the case of a left nephrectomy, using an extraperitoneal approach, where possible, is the best way of reducing splenic injury.[12] It is crucial to remember the aphorism "Pray before surgery, but remember the God will not alter a faulty incision." (Arthur H. Keeny) and plan an appropriate incision. A ′re-do′ anti-reflux procedure may be easier and safer via a thoracic approach. Similarly, a thoraco-abdominal incision can be planned, instead of a abdominal incision alone, for a difficult time and consuming left hypochondrium surgical procedure. "Big surgeons make big (correct) incision", holds true even today in the era of modern surgery. Prophylactic division of the splenoperitoneal folds
Early prophylactic division of the splenoperitoneal folds ensures that there is no untoward traction to various splenic folds.[4],[5],[15],[16],[17],[20],[35],[36] [Figure
- 2] and [Figure - 3].
Avoid unnecessary traction near spleen
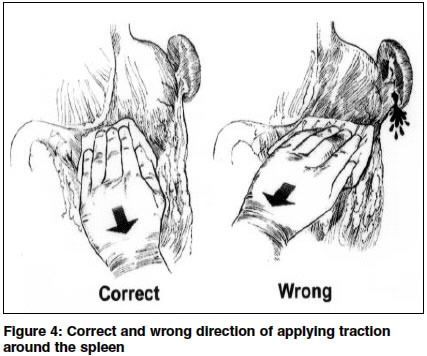
Traction over spleen when required should be minimized by the well-known technique of keeping a large moist pack behind the spleen.[32] Exercising cautious traction, especially ensuring proper direction of traction in operations in the left hypochondrium is another key to avoid accidental splenic trauma. Medial traction on the lieno-omental and lieno-gastric bands and downward traction on the lieno-colic band should be avoided at all costs.[37] [Figure
- 4]. The use of metal clips to secure the short gastric vessels during upper gastrointestinal surgery is a safe way of avoiding undue traction on the stomach.[5]
Optimize visualization
In an attempt to optimize visualization, while mobilizing splenic flexure of colon, surgeons have positioned the patients in a modified lithotomy position and stood between the legs of the patient.[17] Use of fiber-optic light cable can optimize illumination of the operation field. The superiority of visualization as obtained at laparoscopic surgery is confirmed by significantly lower incidence of splenic injury during laparoscopic surgery as seen in fundoplication.[38],[39] Careful use of retractors
Use of rigid retractors must be avoided in re-operations especially in elderly people, or where there is suspicion of intrinsic splenic abnormality.[18],[33] Judicious and gentle use of self-retaining subcostal and manual retractors goes a long way in avoiding iatrogenic trauma to spleen.[5],[8] Splenic flexure mobilization40,41
Mobilization of the splenic flexure is best performed by the surgeon operating from the right side of the patient with first assistant standing between the patient′s legs, which maximizes his view and ability to assist. A second assistant on the left side of the retracts the wound and the left costal margin. It is for this part of the operation that the incision in the upper part of wound should be adequate. The first three steps in the mobilization are:
1. Release of omental adhesions to the anterior border of spleen.
2. Release of omental adhesions to the left paracolic gutter at the level of lower pole of spleen.
3. Division of peritoneum between the colon and the lower border of spleen. These three manoeuvres release the spleen and effectively prevent traction injury to splenic capsule. It is important not to pull down on the descending colon because this can result in splenic injury; instead the thrust of dissection is upwards towards the splenic flexure. One must remember that the spleno-colic ligament is often quite thick and may require division between clamps and transfixing suture ligation. Corman suggests putting only one clamp on the splenic side to avoid tearing the splenic capsule; and dividing the spleno-colic ligament on the flexure side.[42] If the splenic flexure is difficult to expose, it is helpful to enter the lesser sac in the midline and approach the spleno-colic ligament from both the sides: along the left transverse colon from within the lesser sac and along the descending colon in the retroperitoneum. Constant awareness of the continued prevalence of this operative complication and the mechanisms by which it is produced has enabled surgeons to lessen its frequency and potential sequelae.[16] Laparoscopic surgery and iatrogenic splenic injuries
Laparoscopic surgery, with all of its modern technology, is no panacea and has its share of iatrogenic splenic injuries during various procedures like laparoscopic nephrectomy, fundoplication, adrenalectomy etc.[43],[44],[45],[46] The reasons are same as in conventional surgery e.g. traction injuries of splenic ligaments and adhesions and very rarely direct trocar injuries. Rarely, even a simple diagnostic laparoscopy and induction of pneumoperitoneum can result in tearing away of delicate peritoneal reflections or small adhesions on the splenic capsule leading to sudden rupture and hemorrhage.[47] But, by and large, superior visualization obtained at laparoscopic surgery should also result in a decrease in the incidence of iatrogenic splenic injuries. Another advantage is that an experienced laparoscopic surgeon can identify and repair the injury intra-operatively, laparoscopically, minimizing patient morbidity postoperatively.[48] Treatment of iatrogenic splenic trauma
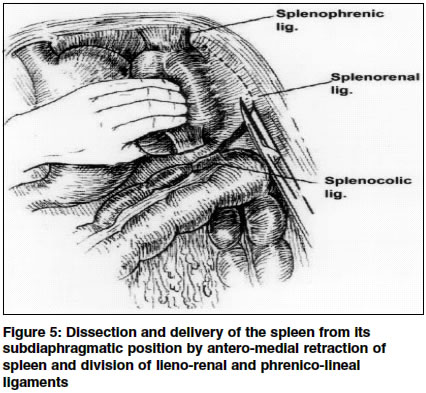
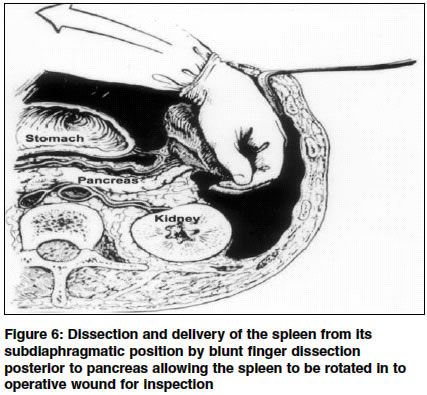
An unexplained pool of blood in the left hypochondrium should alert the surgeon to the possibility of iatrogenic splenic trauma. Immediate dissection and delivery of the spleen from its subdiaphragmatic position is the first step, thus avoiding further iatrogenic injuries, which can readily occur in such an emergency situation.[49],[50] [Figure
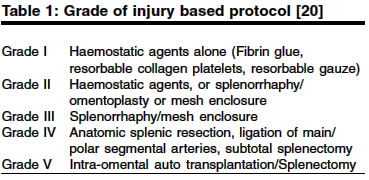
- 5] and [Figure - 6]. The hilus is then clamped with a non-crushing vascular or intestinal clamp, which avoids blood loss during the examination of severity of trauma. Good visualization of the trauma site can be obtained by complete removal of clot by gentle irrigation. The methods used for the repair are well known and depend on the grade of the injury.[51] [Table
- 1]. Clearly, the more extensive the injury to the spleen the more difficult it is to preserve. Post-operatively radiocolloid spleen scan for assessment of function and healing may be done but is not required for grade I-III as there are no late failures of repair.[52] Close to 75% of all accidentally injured spleens can be safely salvaged. If the splenic injury is promptly recognized and managed properly, then the outcome is not adversely affected by such a mishap. A careful examination of spleen at the end of operative procedure should be done to insure that an inadvertent injury is not missed on table. However, when missed on table, some cases require reoperation for control of continued bleeding from unrecognized iatrogenic splenic trauma.[16] More than expected blood from the drain and/or unexpected hypotension in the post-operative period should alert the surgeon to this problem.
Contraindications to salvaging accidentally injured spleen
Contraindications to salvaging accidentally injured spleen are preexisting splenic disease, subject on anticoagulants (vascular operations), labile blood pressure, multiple intra-abdominal lesions, presence of intra-peritoneal infection, age over 70 years.[8],[53] Lack of post-operative monitoring facilities makes the splenic conservation difficult and possibly even dangerous. In some patients, irreparably injured organ or instability of the patient′s condition may demand prompt splenectomy rather than spending time on futile efforts for splenic conservation with its attendant risk of excessive blood loss.
REFERENCES
| 1. | Roy M, Geller JS. Increased morbidity of iatrogenic splenectomy. Surg Gynecol Obstet 1974;139:392-4. Back to cited text no. 1 [PUBMED] |
| 2. | Walstad PM. Operative trauma to the spleen: Incidence, morbidity and mortality. Am Surg 1974;40:586-90. Back to cited text no. 2 [PUBMED] |
| 3. | Danforth DN Jr, Thorbjarnarson B. Incidental splenectomy: A review of the literature and the New York Hospital experience. Ann Surg 1976;183:124-9. Back to cited text no. 3 [PUBMED] |
| 4. | Morgenstern L. The avoidable complications of splenectomy. Surg Gynecol Obstet 1977;145:525-8. Back to cited text no. 4 [PUBMED] |
| 5. | Rogers DM, Herrington JL Jr, Morton C. Incidental splenectomy associated with Nissen fundoplication. Ann Surg 1980;191:153-6. Back to cited text no. 5 [PUBMED] |
| 6. | Pate JW, Peters TG, Andrews CR. Postsplenectomy complications. Am Surg 1985;51:437-41. Back to cited text no. 6 [PUBMED] |
| 7. | Konstadoulakis MM, Kymionis GD, Leandros E, Ricaniadis N, Manouras A, Krespis E, et al. Long term effect of splenectomy on patients operated on for cancer of the left colon: A retrospective study. Eur J Surg 1999;165:583-7. Back to cited text no. 7 [PUBMED] |
| 8. | Eaton MA, Valentine J, Jackson MR, Modrall G, Clagett P. Incidental splenic injury during abdominal vascular surgery: A case-controlled analysis. J Am Coll Surg 2000;190:58-64. Back to cited text no. 8 [PUBMED] [FULLTEXT] |
| 9. | Coltheart G, Little JM. Splenectomy: A review of morbidity. Aust N Z J Surg 1976;46:32-6. Back to cited text no. 9 [PUBMED] |
| 10. | Fabri PJ, Metz EN, Nick WV, Zollinger RM. A quarter century with splenectomy. Changing concepts. Arch Surg 1974;108:569-75. Back to cited text no. 10 [PUBMED] |
| 11. | Fujita T, Matai K, Kohno S, Itsubo K. Impact of splenectomy on circulating immunoglobulin levels and the development of postoperative infection following total gastrectomy for gastric cancer. Br J Surg 1996;83:1776-8. Back to cited text no. 11 [PUBMED] |
| 12. | Cassar K, Munro A. Iatrogenic splenic injury. J R Coll Surg Edinb. 2002;47:731-41. Back to cited text no. 12 [PUBMED] |
| 13. | Rich NM, Lindner HH, Mathewson C Jr. Splenectomy incidental to iatrogenic trauma. Am J Surg 1965;110:209-15. Back to cited text no. 13 |
| 14. | Rose AT, Newman MI, Debelak J, Pinson CW, Morris JA Jr, Harley DD, et al. The incidence of splenectomy is decreasing: Lessons learned from trauma experience. Am Surg 2000;66:481-6. Back to cited text no. 14 [PUBMED] |
| 15. | Hugh TB, Coleman MJ, Cohen A. Splenic protection in left upper quadrant operations. Aust N Z J Surg 1986;56:925-8. Back to cited text no. 15 [PUBMED] |
| 16. | Coon WW. Iatrogenic splenic injury. Am J Surg 1990;159:585-8. Back to cited text no. 16 [PUBMED] |
| 17. | Langevin JM, Rothenberger DA, Goldberg SM. Accidental splenic injury during surgical treatment of the colon and rectum. Surg Gynecol Obstet 1984;159:139-44. Back to cited text no. 17 [PUBMED] |
| 18. | Peters TG, Steinmetz SR, Cowan GS Jr. Splenic injury and repair during bariatric surgical procedures. South Med J 1990;83:166-9. Back to cited text no. 18 [PUBMED] |
| 19. | Cooper CS, Cohen MB, Donovan JF Jr. Splenectomy complicating left nephrectomy. J Urol 1996;155:30-6. Back to cited text no. 19 [PUBMED] |
| 20. | Mejean A, Vogt B, Quazza JE, Chretien Y, Dufour B. Mortality and morbidity after nephrectomy for renal cell carcinoma using a transperitoneal anterior subcostal incision. Eur Urol 1999;36:298-302. Back to cited text no. 20 [PUBMED] [FULLTEXT] |
| 21. | Klaue P, Eckert P, Kern E. Incidental splenectomy: Early and late postoperative complications. Am J Surg 1979:138:296-300. Back to cited text no. 21 |
| 22. | Peck DA, Jackson FC. Splenectomy after surgical trauma. Arch Surg 1964; 89:54-64. Back to cited text no. 22 |
| 23. | Orringer MB, Marshall B, Iannettoni MD. Transhiatal esophagectomy: Clinical experience and refinements. Ann Surg 1999;230:392-403. Back to cited text no. 23 |
| 24. | Katariya K, Harvey JC, Pina E, Beattie EJ. Complications of transhiatal esophagectomy. J Surg Oncol 1994;57:157-63. Back to cited text no. 24 [PUBMED] |
| 25. | Polk HC. Fundoplication for reflux esophagitis: Misadventures with the operation of choice. Ann Surg 1976;183:645-52. Back to cited text no. 25 |
| 26. | Reilly LM, Ramos TK, Murray SP, Cheng SWK, Stoney RJ. Optimal exposure of the proximal abdominal aorta: A critical appraisal of transabdominal medial visceral rotation. J Vasc Surg 1994;19:375-90. Back to cited text no. 26 |
| 27. | Skandalakis PN, Colborn GL, Skandalakis LJ, Richardson DD, Mitchell WE, Skandalakis JE. The surgical anatomy of the spleen. Surg Clin North Am 1993;73:747-68. Back to cited text no. 27 |
| 28. | Lord MD, Gourevitch A. The peritoneal anatomy of the spleen with special reference to the operation of partial gastrectomy. Br J Surg 1965;52:202-4. Back to cited text no. 28 [PUBMED] |
| 29. | Tocchi A, Fornasari V, Puma F, Di Giorgio A. Embryologic and anatomo-surgical presuppositions in intraoperative injuries of the spleen. A clinical study. Minerva Chir. 1989;44:937-42. [Article in Italian] Back to cited text no. 29 |
| 30. | Devlin HB, Evans DS, Birkhead JS. The incidence and morbidity of accidental injury to the spleen occurring during abdominal surgery. Br J Surg 1969;56:446-8. Back to cited text no. 30 [PUBMED] |
| 31. | Ferraris VA, Sube J. Retrospective study of the surgical management of reflux esophagitis. Surg Gynecol Obstet 1981;152:17-21. Back to cited text no. 31 [PUBMED] |
| 32. | Lieberman RC, Welch C. A study of 248 instances of traumatic upture of the spleen. Surg Gynecol Obstet 1968;127:961-5. Back to cited text no. 32 |
| 33. | Cioffiro W, Schein CJ, Gliedman ML. Splenic injury during abdominal surgery. Arch Surg 1976;111:167-71. Back to cited text no. 33 [PUBMED] |
| 34. | Carmignani G, Traverso P, Corbu C. Incidental splenectomy during left radical nephrectomy: Reasons and ways to avoid it. Urol Int 2001;67:195-8. Back to cited text no. 34 [PUBMED] [FULLTEXT] |
| 35. | Wangensteen SL, Kelly JM. Gastric mobilisation prior to vagotomy to lessen splenic trauma. Surg Gynecol Obstet 1968;127:603-5. Back to cited text no. 35 [PUBMED] |
| 36. | Mejean A, Chretien Y, Vogt B, Cazin S, Balian C, Thiounn N, et al. Coloepiploic mobilization during left radical nephrectomy for renal cell carcinoma is indicated to reduce the risk of iatrogenic splenectomy. Urology 2002;59:358-61. Back to cited text no. 36 [PUBMED] [FULLTEXT] |
| 37. | Morris M, Gershenson DM, Burke TW, Wharton JT, Copeland LJ, Rutledge FN. Splenectomy in gynecologic oncology: Indications, complications and technique. Gynecol Oncol 1991;43:118-22. Back to cited text no. 37 [PUBMED] |
| 38. | Laine S, Rantala A, Gullichsen R, Ovaska J. Laparoscopic vs conventional Nissen fundoplication. A prospective randomised study. Surg Endosc 1997;11:441-4. Back to cited text no. 38 [PUBMED] [FULLTEXT] |
| 39. | Hinder R, Perdikis G, Klinger PJ, DeVault KR. The Surgical option for gastroesophageal reflux disease. Am J Med 1997;103:144-8. Back to cited text no. 39 |
| 40. | Rothenburger DA. Conventional colectomy. In: Fielding LP, Goldberg SM, (Ed). Rob and Smith's Operative surgery: Surgery of the colon, rectum and anus. London: Butterworth-Heinemann Ltd 1993;5:347-58. Back to cited text no. 40 |
| 41. | Killingback M. Elective surgery for sigmoid diverticular disease. In: Fielding LP, Goldberg SM, (Ed). Rob and Smith's Operative surgery: Surgery of the colon, rectum and anus. London: Butterworth-Heinemann Ltd 1993;5:369-86. Back to cited text no. 41 |
| 42. | Corman ML. Carcinoma of colon. In Colon and Rectal Surgery. Philadelphia: JB Lippincott Company 1993;3:487-595. Back to cited text no. 42 |
| 43. | Gill IS, Kavoussi LR, Clayman RV, Ehrlich R, Evans R, Fuchs G, et al. Complications of laparoscopic nephrectomy in 185 patients: A multi-institutional review. J Urol 1995;154:479-83. Back to cited text no. 43 [PUBMED] |
| 44. | Hughes SG, Chekan EG, Ali A, Reintgen KL, Eubanks WS. Unusual complications following laparoscopic Nissen fundoplication. Surg Laparosc Endosc Percutan Tech 1999;9:143-7. Back to cited text no. 44 [PUBMED] |
| 45. | Dahlberg PS, Deschamps C, Miller DL, Allen MS, Nichols FC, Pairolero PC. Laparoscopic repair of large paraesophageal hiatal hernia. Ann Thorac Surg 2001;72:1125-9. Back to cited text no. 45 [PUBMED] |
| 46. | Del Pizzo JJ, Shichman SJ, Sosa RE. Laparoscopic adrenalectomy: The New York-Presbyterian Hospital experience. J Endourol 2002;16:591-7. Back to cited text no. 46 [PUBMED] [FULLTEXT] |
| 47. | Takeuchi K, Yamada T, Sato A, Nakago S, Maruo T. Rupture of the spleen as an unusual complication of laparoscopy. A case report. J Reprod Med 2001;46:779-80. Back to cited text no. 47 [PUBMED] |
| 48. | Canby-Hagino ED, Morey AF, Jatoi I, Perahia B, Bishoff JT. Fibrin sealant treatment of splenic injury during open and laparoscopic left radical nephrectomy. J Urol. 2000;164:2004-5. Back to cited text no. 48 [PUBMED] [FULLTEXT] |
| 49. | Borlase BC, Moore EE, Moore FA. Mobilization of the spleen in splenic salvage. Surg Gynecol Obstet 1988;166:278-80. Back to cited text no. 49 [PUBMED] |
| 50. | Schweizer W, Bohlen L, Gilg M, Blumgart LH. Technical aspects of spleen saving therapy in splenic trauma. Helv Chir Acta 1991;58:137-41. [Article in German] Back to cited text no. 50 |
| 51. | Moore EE, Cogbill TH, Jurkovich GJ, Shackford SR, Malangoni MA, Champion HR. Organ injury scaling: Spleen and liver (1994 revision). J Trauma 1995;38:323-4. Back to cited text no. 51 [PUBMED] [FULLTEXT] |
| 52. | Lyass S, Sela T, Lebensart PD, Muggia-Sullam M. Follow-up imaging studies of blunt splenic injury: Do they influence management? Isr Med Assoc J 2001;3:731-3. Back to cited text no. 52 [PUBMED] |
| 53. | Bahnini J, Meyer C, de Manzini N, Rohr S, Hollender LF. Injuries of the spleen: Conservative treatment or exeresis? Chirurgie 1989;115:45-50. [Article in French] Back to cited text no. 53 |
Copyright 2004 - Indian Journal of Surgery
The following images related to this document are available:
Photo images
[is04036f3.jpg]
[is04036t1.jpg]
[is04036f4.jpg]
[is04036f5.jpg]
[is04036f2.jpg]
[is04036f1.jpg]
[is04036f6.jpg]
|

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}