 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
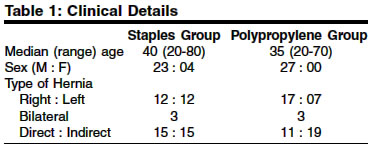
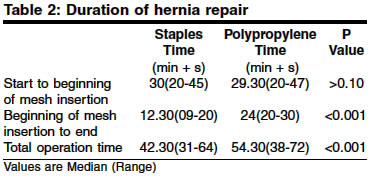
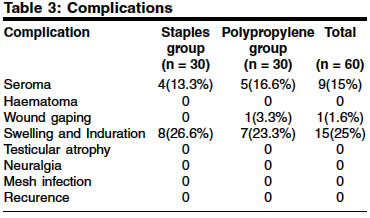
Indian Journal of Surgery, Vol. 66, No. 3, June, 2004, pp. 152-155 Original Article Comparative study of skin staples and polypropylene sutures for securing the mesh in lichtenstein's tension free inguinal hernia repair: A Prospective randomized controlled clinical trial Garg Chaitanya P, Bhatnagar Ashok M, Parmar Chetan D, Darshan Jitendra R, Sehgal Ravi A Department of Surgery, SSG Hospital and Medical College, Baroda Code Number: is04037 ABSTRACT BACKGROUND: The tension-free hernioplasty as introduced by Lichtenstein has gained increasing acceptance during the last decade. This study compared two methods of mesh fixation. MATERIAL AND METHODS: Fifty-four patients undergoing sixty repairs were randomized into two groups. In control group polypropylene mesh was secured with 2/0 polypropylene sutures and skin closed with 2/0 polyamide black. In study group polypropylene mesh was secured with skin staples and skin was closed with staples from the same stapler. Duration of the surgery was recorded. RESULTS: The operation was significantly shorter when staples were used (median 42 min 30 s versus 54 min 30 s, P < 0.001). There was no significant difference in the incidence of postoperative complications or pain. There were no recurrences in either group in the follow up period (median 12 months). CONCLUSION: This technique of mesh fixation is as effective as conventional fixation with polypropylene sutures with an important added advantage; significant reduction in the operative time.INTRODUCTION The Lichtenstein repair is a tension-free inguinal hernia repair which takes account of the important factors identified in the successful outcome of inguinal hernia operation-supplementing the strength of transversalis fascia without disturbing the anatomy and a tension free repair.[1],[2] The standard way of securing the mesh in position on the posterior wall of the inguinal canal is with polypropylene sutures. This trial was conducted to assess the efficacy of anchoring the mesh in position with skin stapler which is quicker when used and should reduce operative time and deal with the problem of wound infection by minimizing the risk of wound colonisation. Thus with this aim we have undertaken this comparative study of skin staples and polypropylene mesh for securing the mesh in Lichtenstein "Tension Free" Inguinal Hernioplasty. MATERIAL AND METHODS This study was carried out in the Department of Surgery SSG Hospital between July 1999 to June 2002. Fifty-four adult patients (> 18 yrs) with primary inguinal hernias were entered into the trial. Informed consent was obtained. All were elective repairs. Patients were randomized either to the staples group (where the mesh was secured with staples) or the polypropylene group (where the mesh was sutured with polypropylene sutures). Three patients in each group underwent bilateral inguinal hernia repair thus making 30 mesh repairs in each group. Most of the operations (n-59) were done under spinal anaesthesia. A single dose of intravenous cefotaxime 1 g was administered 1 hour prior to surgery.Direct hernia sacs were plicated unless very small, when they were reduced unopened. Small indirect sacs were dissected from the spermatic cord and then divided, transfixed and distal part excised. A sheet of polypropylene mesh (11 x 6 cm) was cut to shape and laid over the posterior wall of the inguinal canal so that it overlapped the pubic tubercle by at least 1 cm medially, extended superiorly to lay over the conjoint tendon and to a point at least 2 cm lateral to the internal ring. In the polypropylene group this was fixed in position by interrupted sutures of 2/0 Prolene (Ethicon) along the inguinal ligament inferiorly from the pubic tubercle to the lateral edge of the mesh. Interrupted polypropylene sutures were then placed medially and superiorly into the internal oblique and transversalis muscles. The spermatic cord was passed through a slit in the mesh. Lateral to it the overlapping free edges of the mesh were sutured together with two interrupted polypropylene sutures. In the stapler group the positioning of the mesh was identical but a Proximate Plus MD (multidirectional) release Skin Stapler (Ethicon) containing 35 preloaded stainless steel staples, was used to secure it. A staple was placed into the pubic tubercle with between seven and nine staples along the inguinal ligament placed 1-2 cm apart. A further four to five staples were placed in the internal oblique and transversalis muscle medially and superiorly and the overlapping free edges of the mesh were stapled together with two staples lateral to the cord. In both groups the external oblique aponeurosis was closed with a continuous suture of 2/0 Prolene (Ethicon) and the subcutaneous tissue were then approximated with plain catgut. Skin closure was completed in the polypropylene group using interrupted sutures of 2/0 Ethilon (Ethicon), which were removed 7 days after surgery. In the stapler group skin closure was completed using staples from the same staple gun and these were removed 7 days after operation. The time taken from the skin incision to the beginning of the mesh fixation and from the beginning of the mesh insertion to completion of skin closure was recorded to the nearest 30 seconds. Patients were observed for 4-6 hours until they had emptied their bladders, and were discharged home when considered safe. Some patients were kept in hospital overnight for social, as opposed to surgical reasons. Patients were reviewed in outpatient clinic 7 days after surgery, for stitch/clip removal and information concerning wound complications, duration of pain and return to normal activities. Complications were characterised as infection [defined as requirement for antibiotics for wound infection, urinary tract infection or epididymitis], hematoma requiring drainage or inpatient admission, pain significant to cause alteration in lifestyle, non-infectious urinary complications including acute urinary retention that prolonged hospitalisation, postoperative ileus and other miscellaneous complications. Statistical analysis was performed using the students unpaired "t" test. Patients were followed up at 1 month, 3 months, 6 months, 9 months, 1 year and then at 6 months interval and evaluated for neuralgia and recurrence at each follow-up. Some patients were reminded by post to come to the hospital for follow-up. RESULTS Clinical Details The maximum number of patients (n-24) were in 31-40 age group. There were four female patients in stapler group. Overall 30 repairs were done in each group. Duration of Surgery The median duration of operation in the staples group was 42 min 30 sec compared with 54 min 30 sec in the polypropylene group [Table - 2]. This difference was accounted for by the difference in time from the beginning of the mesh insertion to the end of the operation. The difference in time from the start of surgery to insertion of mesh was not significant (P>0.10) between both groups, but the difference in time from mesh insertion to completion of surgery between the two groups was significant (P<0.001). The difference in total operative time between the two groups was also significant (P<0.001). Postoperative Course The median duration of pain was the same (2 days) in both the groups. The stapler group returned to work at median 12 days compared with 14 days in polypropylene group. This difference was statistically insignificant. Complications There were no cases of mesh infection. There were no hernia recurrence during the follow up period in either group. Follow Up DISCUSSION Egger et al[3] first reported the use of skin staples for securing the mesh in hernia repair. Janu et al[4] reported duration of surgery as "operating room time" of 111+/- 2 min. The results in his series were achieved in the setting of a surgical residency program with a steady turn over of residents being instructed in the Lichtenstein′s mesh plasty technique, without the use of staples. Mills et al[5] reported a similar study to compare skin staples and polypropylene sutures for securing the mesh in inguinal hernioplasty. He reported fifty elective, unilateral, primary inguinal hernia repair done under general anaesthesia. In our study the median length of operation was almost 12 min shorter when staples were used whereas it was 10 minutes shorter in Mills′ study. According to Mills this difference maybe important because shorter operations maybe associated with a reduced risk of wound infection and because this keeps the risk of anaesthesia to a minimum. The use of stapling pins for securing the mesh and closure of skin saved considerable operative time and accounted for the difference of 12 minutes (P<0.001) between the stapler group and polypropylene group. In this study the stapler used was a Proximate Plus MD (multidirectional) release skin stapler. The staples are made from stainless steel with an inert coating. The length of the prongs on the staples is 3.9 mm, which appears sufficient to provide good penetration into the tissue, with secure fixation of the mesh. Mills had used a Proximate RH (Rotating Head) skin stapler in which accurate staple placement is facilitated by the design of the stapler, whose head rotates 360 degrees, thereby allowing maximum visibility and improved access. In our study none of the 36 patients treated as day case surgery required more than one intra muscular analgesic postoperatively. The Royal College of Surgeons of England[6] has suggested that to qualify for day case surgery, patients should not require parenteral analgesia after discharge. The implications of day case treatment and early ambulation are considerable. There was no difference in pain duration in both the groups of our study. Similar results were observed by Mills et al. No cases of neuralgia were observed in our study. Patients in study group reported that they returned to normal activities earlier than those in control group. The median days of return to work were 12 days in stapler group and 14 days in polypropylene group, compared with 24 days and 38 days reported by Mills et al. The difference in return to work in our study was not significant (P>0.10). Early return to work has important implications on the hospital as well as the society in terms of man- power and costs. The main complications in our study were seromas (15%) and transient swelling and induration of wound (25%). There were no differences in complications between staples group and polypropylene group. Mills reported four haematomas, which were not encountered in our study. Concerns had been expressed, that the use of staples may lead to entrapment neuropathy[7],[8] increased rate of wound infection[12] and potential vascular injury.[7],[9],[10] But, no such complications were encountered in this study. There were no recurrences in our study with the follow up of 3-24 months. Mills study also had a short follow up (12 weeks) and no recurrences. CONCLUSIONS The technique of Lichtenstein tension-free repair is simple, relatively easier to learn and less technically demanding as compared to other methods of inguinal hernia repairs, particularly the Shouldice Repair which has until recently been the gold standard recommended by the Royal College of Surgeons of England. A different way of securing the polypropylene mesh, as described by Egger, has been used in our study. The staples placement was done by a routine skin stapler, providing good penetration into the tissues, including the pubic tubercle, with secure fixation of the mesh, making this method technically easier. This study demonstrates that this technique of mesh fixation is as effective as conventional fixation with polypropylene sutures with an important added advantage; significant reduction in the operative time, although in our set-up the cost of consumables per operation is increased when both mesh and staples are used this cost should be carefully weighed against the more efficient use of operative time. This study needs to be evaluated further in a larger group of patients to explore the impact of reduced operative time on post-operative complications and recurrence rate. REFERENCES
Copyright 2004 - Indian Journal of Surgery The following images related to this document are available:Photo images[is04037t2.jpg] [is04037t3.jpg] [is04037t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}