 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
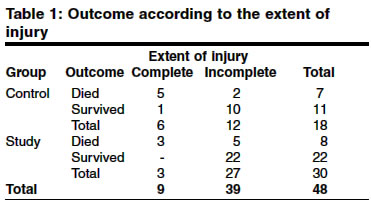
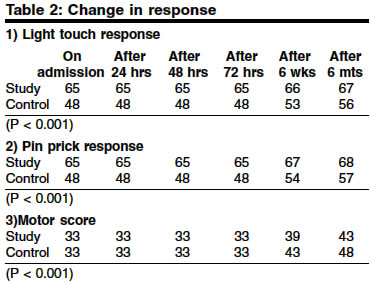
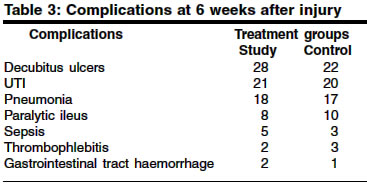
Indian Journal of Surgery, Vol. 66, No. 3, June, 2004, pp. 156-159 Original Article Role of methylprednisolone in acute cervical cord injuries Rasool Tahir , Wani MA, Kirmani Altaf R, Ramzan Altaf U, Wani Rauf Ahmad , Imtiyaz Syed , Batool Gilani Z Department of Neurosurgery, Sher-i-Kashmir Institute of Medical Sciences, Srinagar Code Number: is04038 ABSTRACT BACKGROUND: Management of acute cervical cord injury with neurodeficit continues to evoke debate. Glucocorticoid steroid methylprednisolone has been found to be effective in preventing secondary cord injury. Aims: This study was done to evaluate the role of methylprednisolone in acute cervical cord injury. MATERIAL AND METHODS: Thirty patients of acute cervical cord injury with demonstrable neurological deficit were administered methylprednisolone within 8 hours of acute cervical cord injury while eighteen others were not administered this drug. The patients were assessed for neurological recovery. RESULTS: Patients who received methylprednisolone within 8 hours of injury had more motor recovery (P<0.001) than those who were not given the drug. Improvement in the pinprick scores and light touch scores were also greater at 6 weeks (P<0.001). Similar effect was also seen after 6 months. CONCLUSION: Methylprednisolone prevents secondary cord injury to a great extent and hence its administration in the immediate post injury period results in a better functional (motor and sensory) outcomeINTRODUCTION Traumatic spinal cord injury is a formidable challenge for the injured, for the treating team, for family and friends, and for the society as a whole. It is not so uncommon and worldwide incidence is 9.2-50 patients per million population per year. The cervical spine is the site of injury in 37-55%, the majority occurring between C4 and C6 level, as the cervical canal is narrowest at this level. In the West and industrialized world, road traffic accidents account for 36% to 57% of this type of injury. However, in our region, mostly the injuries are due to fall from trees, horses, bicycles etc., sporting accidents and slips from mountain tops besides road traffic accidents. In addition to primary mechanical injury, the spinal cord undergoes secondary injury by a variety of pathological processes, including ischemia, calcium influx, lipid peroxidation, excitotoxic mechanisms and free radical activation. Methyl prednisolone, the glucocorticoid steroid has been shown to be effective in enhancing neurological recovery in acute spinal cord injury.[1] High doses of methylprednisolone preserves the cord ultrastructure through a reduction of injury-induced, free radical catalyzed lipid peroxidation, when given within eight hours after injury. Patients treated with methyl prednisolone show significant improvement when followed at six weeks and six months after the injury as compared to the patients who did not receive the drug.[2] MATERIAL AND METHODS Forty eight patients of acute cervical cord injury with demonstrable neurological deficit (motor or sensory) were included in this study which was conducted in the department of neurosurgery, SKIMS, Srinagar over a period of two years. Following patients were excluded from the study. a) Patients less than 13 years of age After detailed history and examination, baseline investigations were carried out. Plain radiographs, CT scan, myelogram, myelo CT and MRI were the imaging modalities used for the diagnosis wherever indicated. The neurological function was assessed according to the American Spinal Injury Association (ASIA) scoring system on admission, after 24 hours,. 48 hours, 72 hours, 6 weeks and 6 months after injury. Measurements of motor function and sensations of pinprick and light touch were recorded at each examination. Motor function was evaluated in 14 muscle segments and scored as 0 (No contraction) to 5 (normal power). Expanded motor scores ranged from 0 (no contraction in any muscle segments) to 70 (all normal responses) and were obtained separately for the right and left sides. Pinprick and light touch sensations were evaluated bilaterally in 29 segments from C2 to S5 and their function assessed and scored as 1 (absent), 2 (decreased), or 3 (normal). An expanded score for each measurement ranged from 29 (absent at all levels) to 87 (normal at all levels). After obtaining consent, methylprednisolone was administered in a bolus intravenous dose of 30mg/kg body weight over a ten minute period followed by a maintenance dose of 5.4 mg/kg/hr infusion afterwards for next 23 hours to the patients who present within 8 hours of injury to the hospital. The patients who presented later than 8 hours of injury were placed in the control group (18 patients). RESULTS A total of 48 patients were included in the study, out of which 30 patients were given methylprednisolone and put in the study group and 18 patients were put in the control group. Males constituted almost 80% of the total study population with a predominance of patients lying in the 30-40 year age group (33%) and the commonest mode of injury being falls from trees, mountain tops, stairs, bicycles (77%). 6 patients in control group and 3 in study group had complete cord injury [Table - 1]. The commonest orthopaedic injury was dislocation of C5-C6 vertebra (33%), followed by C6-C7 dislocation (29%) and about 20% patients presented with complete cervical cord injury. Patients who received methylprednisolone within 8 hours of injury had more motor recovery (10.0 vs 6.0; P < 0.001) than those who were not given the drug. Improvement in pinprick scores (7.0 vs 2.0; P < 0.001) and light touch scores (5.0 vs 1.0; P < 0.001) were also greater at 6 weeks. After six months, patients who received methylprednisolone recovered more motor (15.0 vs 10.0; P < 0.001) and sensory function (pinprick l0 vs 3.0; P < 0.001 and touch 8.0 vs 2.0; P < 0.001) than those in the control group [Table - 2]. The commonest complication was decubitus ulcers followed by urinary tract infections (catheter induced) and pulmonary complications [Table - 3]. DISCUSSION After the traumatic event, in addition to the primary mechanical injury, the spinal cord undergoes secondary injury by a variety of pathological processes. There has been a great deal of discussion as to which treatment course is most helpful in ensuring maximum neurologic improvement after a cervical spinal cord injury. Interest in the pharmacologic treatment of acute spinal cord injury dates back to thirty years. The NASCIS (The National Acute Spinal Cord Injury study) was established in 1975 to evaluated pharmacologic therapies in the first hours after a spinal cord injury. In an earlier trial (NASCIS-I), a comparison of a 1000 mg infusion of methylprednisolone sodium succinate with a 100 mg dose of methylprednisolone given as a bolus and daily thereafter for a 10 days was conducted.[3] When NASICS-I study was heading for conclusion, the next trial NASCIS-II, was undertaken to study the response to the higher doses of the glucocorticoid, methylprednisolone (30 mg/kg body weight).1 A placebo arm was added to NASCIS-II, and a second therapeutic candidate, the opiate receptor blocker Naloxone hydrochloride, was added as a third treatment arm. In 1997, NASCIS-III trial was conducted to compare the efficacy of methylprednisolone administered for 24 hours with methylprednisolone administered for 48 hours or tirilazad mesylate (a potent lipid peroxidation inhibitor) for 48 hours.[4] In our study, we administered methylprednisolone to the patients of acute cervical cord injury who presented to the department of Neurosurgery, SKIMS within 8 hours of their injury. Patients who presented late were kept in the control group. After receiving methylprednisolone, no appreciable acute change was noted in any of the responses. However, considering all the patients six weeks after injury, we found that the scores of those treated with methylprednisolone improved more than the scores of those in the control group. The patients in the study group had significant improvement than those in the control group in their motor function (10.0 vs 6.0; P < 0.001) and touch (5.0 vs 1.0; P < 0.001). Improvement in pinprick scores were also greater (7.0 vs 2.0; P < 0.001). After six months, the patients in the study group continued to have greater improvement both in the sensory as well as motor functions. Patients in the study group recovered more motor function than those in the control group (15.0 vs 10.0; P < 0.001). Patients in the study group also had greater sensory recovery (pin prick 9.0 vs 3.0; P < 0.001) and touch, 8.0 vs 2.0; P < 0.001). In view of the statistical analysis of our observations we hypothesize that in patients of acute cervical cord injuries treatment with methylprednisolone results in a significant improvement in motor function and the sensations of pinprick and touch six weeks and six months after the injury. The beneficial effects of methylprednisolone were limited to the patients treated within eight hours of their injury. Patients with either complete or incomplete injuries improved more after treatment with methylprednisolone than without it. The dose of methylprednisolone used in the current study far exceeds the dose necessary to activate corticosteroid receptors. This suggests that methylprednisolone may act through mechanisms unrelated to corticosteroid receptors. High doses of methylprednisolone markedly enhance the flow of blood in injured spinal cords, preventing the typical decline in white-matter blood flow, extracellular calcium levels and evoked potentials that occur after spinal cord injury.[2],[5],[6] The most likely explanation for the observed effects of treatment is that methylprednisolone suppresses the breakdown of membrane by inhibiting lipid peroxidation and hydrolysis at the site of injury. The doses required for a treatment effect are similar to those shown to be most effective in inhibiting lipid peroxidation and breakdown of neurofilament in injured spinal cord.[7] These events in the breakdown of membrane begin and peak within eight hours of injury. A secondary effect of the inhibition of lipid peroxidation is that vasoreactive by-products of arachidonic acid metabolism are reduced, which improves the flow of blood at the injury site. Thus, we conclude that methylprednisolone has an important role in acute cervical cord injury. By preventing lipid peroxidation and stabilizing membranes, it prevents secondary cord injury and hence neuronal degeneration which results in profound motor and sensory loss. Initiated immediately after cord injury, treatment with the glucocorticoid can make a huge difference in the functional outcome of the patients. REFERENCES
Copyright 2004 - Indian Journal of Surgery The following images related to this document are available:Photo images[is04038t3.jpg] [is04038t2.jpg] [is04038t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}