 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
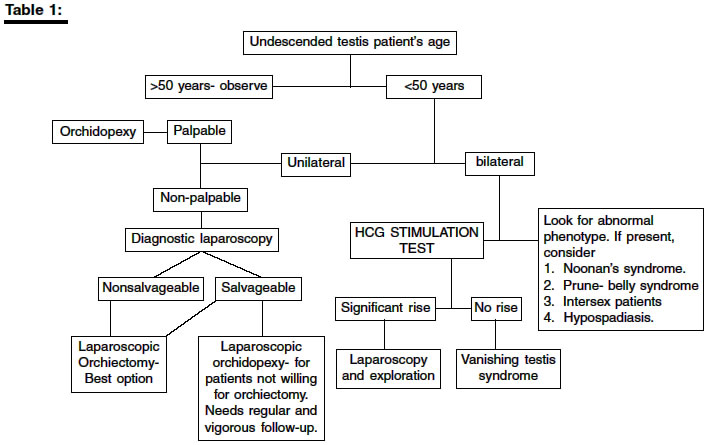
Indian Journal of Surgery, Vol. 66, No. 3, June, 2004, pp. 160-163 Original Article Adult cryptorchidism: Unrevealing the cryptic facts Raghavendran Maniyur , Mandhani Anil , Kumar Anant , Chaudary Himanshu , Srivastava Avinash , Bhandari Mahendra , Dubey D, Kapoor R Department of Urology and Renal Transplantation, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow Code Number: is04039 ABSTRACT BACKGROUND: The incidence of cryptorchidism is 3.7% at birth and by 1 year of age, the incidence declines to about 1% and remains constant thereafter in life. The standard age at which cryptorchid testis is to be corrected is 18 months. In our routine practice, many patients present late in their life with significant risk of malignancy and infertility. AIMS: We tried to evaluate the causes of late presentation in our population. SETTINGS AND DESIGN: To diagnose the true causes late presentation for orchidopexy, a questionnaire-based study was conducted on all adult cryptorchids operated in our institute over a 15 year period. The questionnaire is attached as addendum. MATERIAL AND METHODS: Thirty-three adult cryptorchid patients operated in our institute over a 15-year period (1988-2002), included in this retrospective study. RESULTS: We found that only 9% (3/33) of the patients didn't present due to ignorance. The rest 91% (30/33) knew about their missing testis in childhood. Of these, 14 patients did not present due to shyness while the other 16 had consulted a rural practioners; surprisingly 8 of these 16 patients were not guided further. Five of the twelve patients with bilateral cryptorchidism had infertility. Of the four patients who presented with malignancy, one died during the course of treatment. CONCLUSION: The present study revealed that many treating rural practioners and paramedics were equally responsible for the late presentation of the patients. There is a need for thorough physical examination following birth by attending obstetrician, pediatrician and other practicing physicians. An advice for early corrective surgery will go a long way in reducing the complications due to late presentation.INTRODUCTION Undescended testis (UDT) is a common problem encountered in infancy and childhood. It is the most common congenital anomaly at birth.[1] It is a well established fact that definitive treatment should be done before one and half years of age.[2] Some authors have reported that late presentation is due to acquired descent but these reports are isolated.[3] We tried to evaluate the causes of late presentation in our population. We thought that undescended testis is an entity, present since childhood and late presentation is due to shyness, ignorance and lack of awareness of the magnitude of this problem. The omission of diagnosing undescended testis at birth or thereafter is a real cause for concern. Examination of external genitalia is an essential part of the abdominal system examination and is taught to medical students at the beginning of their training. Still we know that many such conditions continue to evade medical attention due to casualness on the part of the treating physician and apathy of the patient towards seeking medical advice earlier. Of the many consequences of untreated cryptorchidism, neoplasia and infertility are the most important. In a series of 52 orchiectomies done in post pubertal males presenting with UDT, only one testis showed normal spermatogenesis with mature spermatozoa and the rest all showed incomplete maturation.[4] Similarly the relative risk of testicular cancer in a cryptorchid testis is 40 times greater than the general population.[5] Orchiopexy allows thorough examination of the testis and theoretically earlier detection of the tumor. We planned a questionnaire based study among our patients who have reached adulthood without getting treatment for undescended testis. The idea was to know the reasons for not reporting in early childhood and to suggest measures to curb the menace of undescended testis presenting in adulthood. MATERIAL AND METHODS A questionnaire based study was conducted among adult cryptorchid patients (age > 18 years), operated in our institute over a 15 year period (1998-2002). These patients were given a questionnaire and answers were elicited from them either during their hospital stay (10 patients) or by mail (23 patients). Questionnaire was addressed to both the children/patients concerned and the parent/guardians. Informed consent was obtained from the patients and the hospital ethical committee had approved the study.Age at presentation, the type of surgery (reconstructive/ablative), laterality, hospital course and morbidity and mortality of the patients presenting due to the complications were recorded. RESULTS There were 33 patients with unilateral (21) and bilateral (12) UDT. The average age at which they came to know of the problem was 5.16 (2-7) years. The average age at which they underwent surgery was 27 years (mean age 15-54 years). The answers obtained by the patients were tabulated and analyzed. In the unilateral group 8 patients underwent orchidopexy, 11 patients underwent orchidectomy and 2 patients had vanishing testis syndrome. In the bilateral group, 8 patients underwent orchidopexy on at least one side and orchiectomy of the contralateral side, one patient underwent right orchiectomy and the left testis could not be localized. 2 patients underwent bilateral orchiectomy for tumors. A single patient sustained mortality before being taken up for surgery due to chemotherapy related problems. Five of the 12 patients with bilateral UDT presented because of infertility. Semen analysis in all the five revealed azoospermia. 4 patients (2 with unilateral and 2 with bilateral UDT) presented with tumors. One patient with unilateral UDT had seminoma and received chemotherapy. The second patient had seminoma and received radiotherapy. He is doing well at 11 years follow-up. Of 2 patients with non-seminoma in bilateral UDT, one patient received chemotherapy initially as there was large volume disease on CT scan. This patient died 1 week after the first cycle due to BEP (Bleomycin, Etoposide, and Cisplatinum) induced mesenteric vein thrombosis and gangrene of small bowel. Ninety one percent (30/33) patients were aware of the missing testis in childhood. Nine percent (3/33) of the patients did not reveal their problem due to complete ignorance. Of the 30 patients, 42% (14/33) did not present to rural practitioners due to shyness. Amongst the other 16 patients who reported to the rural practitioners, 8 were not guided further, and rest 8 did not undergo surgery as they thought that this condition is not giving them any problem. DISCUSSION It has become standard teaching now that the age at which UDT has to be corrected is 18 months to avoid any adverse consequences in the future.[2] Unfortunately many of our patients present late due to various unknown reasons. Often there is an easy explanation for the late presentation, like living in a remote area and non-availability of medical facilities. Occasionally the explanation is obvious but disturbing; that is patient did see a rural practitioner, but was reassured that nothing was wrong. The present study, based on questionnaire pertaining to the reasons for late presentation had revealed some enlightening facts. Undescended testis is usually congenital in origin and late presentation should not be taken as proof for an acquired basis of this disorder as suggested by some authors.[3] We found that 9% of delayed presentation was due to ignorance, meaning that patients did not know about their missing testis and surprisingly one out of these three patients had bilateral undescended testis. 42% of the patients presented late due to shyness. Sixteen patients had consulted a rural practitioner and 8 out of the 1[6] had to suffer because of improper guidance by the attending practitioners. This shows an urgent need for education programme to increase awareness amongst the health workers, individuals and the general public. All these patients could have been diagnosed by simple examination of the genitalia as the presence or absence of testis could easily be noticed by any consulting pediatrician or health worker. Though the entity of retractile testis is well known, most of them descend during early infancy. So an ideal age for detection will be a thorough physical examination at 1 year of age. At this age almost all children consult a pediatrician for multitude of problems. A thorough examination of the genitalia by the pediatrician irrespective of the presenting complaint of the child will go a long way in early diagnosis and treatment of the problem. The treatment of this condition is also simple and straightforward. Laparoscopy was recommended for this condition by Cortesi in 1976 and has progressed from a diagnostic to therapeutic modality.6 When performed by a careful and experienced surgeon, laparoscopy is safe and has few complications. Laparoscopy is by far the most sensitive and specific procedure to localize an undescended testis and to determine whether a gonad is present or absent. Its accuracy rates from 88-100% and is widely used as the first step in the management of nonpalpable testis.[7] It is clear from literature that in a postpubertal patient with undescended testis, efforts should be made to preserve at least one testis if both are undescended and orchidectomy should be done for unilateral cases because these testes cannot produce spermatozoa and have a significant risk of malignant change.[8] In our study we have done salvage orchidopexy even in unilateral cases as the patients were not ready for emasculation and we found no adverse event in the follow-up period. The present study showed that greater the age of the patient, the lesser is the chance of salvagibility. Unlike unilateral UDT, bilateral UDT is associated with significant risk of infertility which otherwise is correctable. Five patients in the bilateral group (41%) presented due to infertility. In the infertile population, we could not do any corrective surgery and all the patients had to resort to adoption or an artificial reproduction technique (ART). An even more dangerous trend was the high number of tumors seen in persistent undescended testis. A study from Delhi had shown that 14% of adult patients with germ cell tumor had cryptorchidism.[9] The incidence among adult cryptorchid patients has not been reported till date. These tumors behave differently when compared to the tumors in descended testis. The mortality and morbidity could not be compared due to the small number of cases in our study, but still these cases merit a discussion. It has been shown that patients presenting within one month of noticing testicular malignancy have a very high chance of cure with orchidectomy alone.[10] Treatment delay of more than 3 months has been associated with significantly decreased five-year survival.[11] Invariably malignancy in cryptorchidism presents late due to delayed clinical features. Early diagnosis and correction of the problem will go a long way in decreasing the morbidity and mortality. Two of the tumors were associated with bilateral disease. Both these patients knew about their disease since childhood. One patient consulted a practitioner who did not guide properly. This patient underwent abdominal exploration and bilateral orchiectomy[1]. He received chemotherapy and had retroperitoneal lymph node dissection for persistent retroperitoneal nodes after 4 cycles of chemotherapy. The second patient had tumor in unilateral undescended testis. This patient did not undergo any evaluation as he was asymptomatic initially. This patient is luckily doing well after orchiectomy and radiotherapy. The other 2 patients with malignancy did not consult anyone as they were asymptomatic. One presented with abdominal mass and CT scan diagnosed the tumor in undescended testis. In this patient we planned neo-adjuvant chemotherapy due to seemingly unresectable tumor on CT scan, but the patient succumbed to the first cycle of chemotherapy. Before concluding, we would like to mention briefly about the most important advance in the management of the post-pubertal patient with cryptorchidism. Farrer et al in 1985 had recommended surgical intervention be limited to patients 32 years or younger using perioperative and testis cancer mortality data from the 70′s.[12] Since that time, there have been significant improvements in perioperative care and germ cell tumor therapy. Landman et al revisited the topic using contemporary data and advocated orchiectomy in all healthy males who present with postpubertal cryptorchidism until age 50 years.[13] We also follow the policy advocated by Landman. Our algorithm for managing these patients is given in [Table - 1]. CONCLUSION Careful physical examination of the baby at birth, regular follow-up of the infant and advice for early corrective surgery in cases of persistent undescended testis will go a long way in reducing the morbidity and mortality due to cryptorchidism. There is a need for public education programme to encourage testicular self examination and health workers can play a major role in this. Addendum: Questionnaire
REFERENCES
Copyright 2004 - Indian Journal of Surgery The following images related to this document are available:Photo images[is04039t1.jpg] |
| |||||||||

{kind=link}